
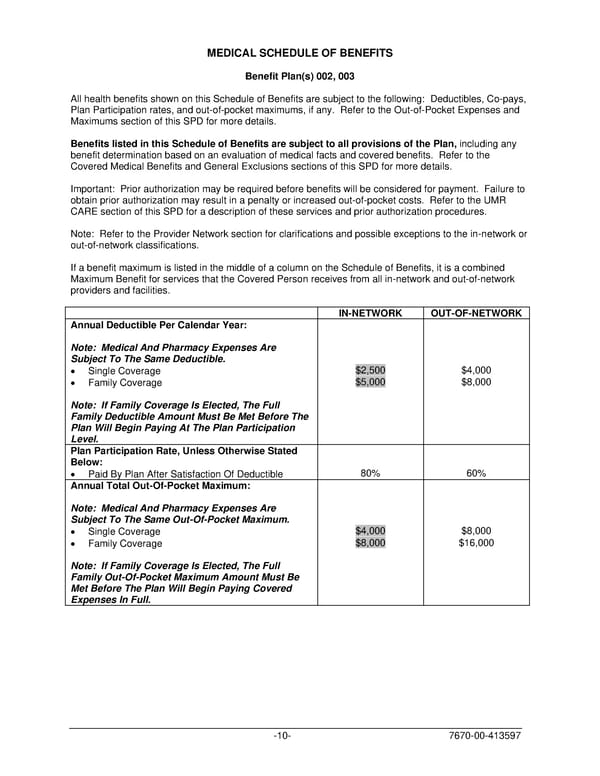
MEDICAL SCHEDULE OF BENEFITS Benefit Plan(s) 002, 003 All health benefits shown on this Schedule of Benefits are subject to the following: Deductibles, Co-pays, Plan Participation rates, and out-of-pocket maximums, if any. Refer to the Out-of-Pocket Expenses and Maximums section of this SPD for more details. Benefits listed in this Schedule of Benefits are subject to all provisions of the Plan, including any benefit determination based on an evaluation of medical facts and covered benefits. Refer to the Covered Medical Benefits and General Exclusions sections of this SPD for more details. Important: Prior authorization may be required before benefits will be considered for payment. Failure to obtain prior authorization may result in a penalty or increased out-of-pocket costs. Refer to the UMR CARE section of this SPD for a description of these services and prior authorization procedures. Note: Refer to the Provider Network section for clarifications and possible exceptions to the in-network or out-of-network classifications. If a benefit maximum is listed in the middle of a column on the Schedule of Benefits, it is a combined Maximum Benefit for services that the Covered Person receives from all in-network and out-of-network providers and facilities. IN-NETWORK OUT-OF-NETWORK Annual Deductible Per Calendar Year: Note: Medical And Pharmacy Expenses Are Subject To The Same Deductible. • Single Coverage $2,500 $4,000 • Family Coverage $5,000 $8,000 Note: If Family Coverage Is Elected, The Full Family Deductible Amount Must Be Met Before The Plan Will Begin Paying At The Plan Participation Level. Plan Participation Rate, Unless Otherwise Stated Below: • Paid By Plan After Satisfaction Of Deductible 80% 60% Annual Total Out-Of-Pocket Maximum: Note: Medical And Pharmacy Expenses Are Subject To The Same Out-Of-Pocket Maximum. • Single Coverage $4,000 $8,000 • Family Coverage $8,000 $16,000 Note: If Family Coverage Is Elected, The Full Family Out-Of-Pocket Maximum Amount Must Be Met Before The Plan Will Begin Paying Covered Expenses In Full. -10- 7670-00-413597
 PLAN 01 01 2024 00 Page 12 Page 14
PLAN 01 01 2024 00 Page 12 Page 14