
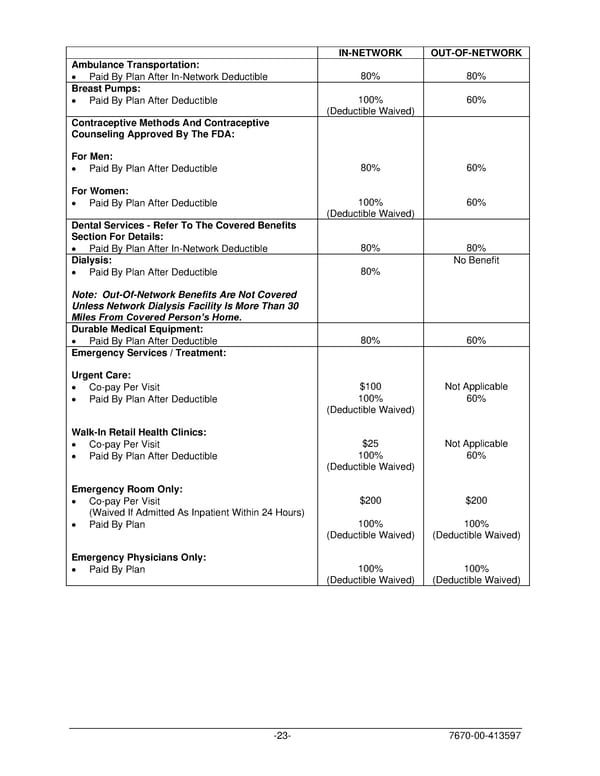
IN-NETWORK OUT-OF-NETWORK Ambulance Transportation: • Paid By Plan After In-Network Deductible 80% 80% Breast Pumps: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Contraceptive Methods And Contraceptive Counseling Approved By The FDA: For Men: • Paid By Plan After Deductible 80% 60% For Women: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Dental Services - Refer To The Covered Benefits Section For Details: • Paid By Plan After In-Network Deductible 80% 80% Dialysis: No Benefit • Paid By Plan After Deductible 80% Note: Out-Of-Network Benefits Are Not Covered Unless Network Dialysis Facility Is More Than 30 Miles From Covered Person’s Home. Durable Medical Equipment: • Paid By Plan After Deductible 80% 60% Emergency Services / Treatment: Urgent Care: • Co-pay Per Visit $100 Not Applicable • Paid By Plan After Deductible 100% 60% (Deductible Waived) Walk-In Retail Health Clinics: • Co-pay Per Visit $25 Not Applicable • Paid By Plan After Deductible 100% 60% (Deductible Waived) Emergency Room Only: • Co-pay Per Visit $200 $200 (Waived If Admitted As Inpatient Within 24 Hours) • Paid By Plan 100% 100% (Deductible Waived) (Deductible Waived) Emergency Physicians Only: • Paid By Plan 100% 100% (Deductible Waived) (Deductible Waived) -23- 7670-00-413597
 PLAN 01 01 2024 00 Page 25 Page 27
PLAN 01 01 2024 00 Page 25 Page 27