
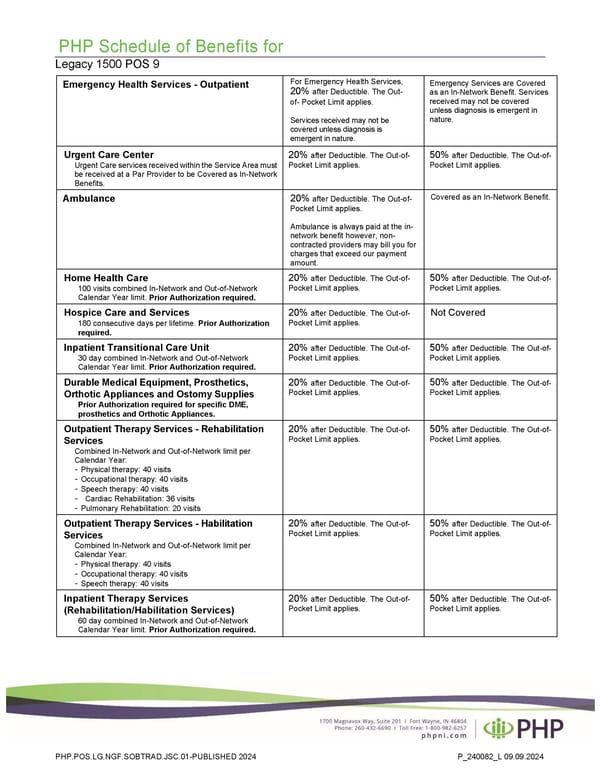
PHP Schedule of Benefits for Legacy 1500 POS 9 Emergency Health Services - Outpatient For Emergency Health Services, 20% after Deductible. The Out- of- Pocket Limit applies. Services received may not be covered unless diagnosis is emergent in nature. Emergency Services are Covered as an In-Network Benefit. Services received may not be covered unless diagnosis is emergent in nature. Urgent Care Center Urgent Care services received within the Service Area must be received at a Par Provider to be Covered as In-Network Benefits. 20% after Deductible. The Out-of- Pocket Limit applies. 50% after Deductible. The Out-of- Pocket Limit applies. Ambulance 20% after Deductible. The Out-of- Pocket Limit applies. Ambulance is always paid at the in- network benefit however, non- contracted providers may bill you for charges that exceed our payment amount. Covered as an In-Network Benefit. Home Health Care 100 visits combined In-Network and Out-of-Network Calendar Year limit. Prior Authorization required. 20% after Deductible. The Out-of- Pocket Limit applies. 50% after Deductible. The Out-of- Pocket Limit applies. Hospice Care and Services 180 consecutive days per lifetime. Prior Authorization required. 20% after Deductible. The Out-of- Pocket Limit applies. Not Covered Inpatient Transitional Care Unit 30 day combined In-Network and Out-of-Network Calendar Year limit. Prior Authorization required. 20% after Deductible. The Out-of- Pocket Limit applies. 50% after Deductible. The Out-of- Pocket Limit applies. Durable Medical Equipment, Prosthetics, Orthotic Appliances and Ostomy Supplies Prior Authorization required for specific DME, prosthetics and Orthotic Appliances. 20% after Deductible. The Out-of- Pocket Limit applies. 50% after Deductible. The Out-of- Pocket Limit applies. Outpatient Therapy Services - Rehabilitation Services Combined In-Network and Out-of-Network limit per Calendar Year: - Physical therapy: 40 visits - Occupational therapy: 40 visits - Speech therapy: 40 visits - Cardiac Rehabilitation: 36 visits - Pulmonary Rehabilitation: 20 visits 20% after Deductible. The Out-of- Pocket Limit applies. 50% after Deductible. The Out-of- Pocket Limit applies. Outpatient Therapy Services - Habilitation Services Combined In-Network and Out-of-Network limit per Calendar Year: - Physical therapy: 40 visits - Occupational therapy: 40 visits - Speech therapy: 40 visits 20% after Deductible. The Out-of- Pocket Limit applies. 50% after Deductible. The Out-of- Pocket Limit applies. Inpatient Therapy Services (Rehabilitation/Habilitation Services) 60 day combined In-Network and Out-of-Network Calendar Year limit. Prior Authorization required. 20% after Deductible. The Out-of- Pocket Limit applies. 50% after Deductible. The Out-of- Pocket Limit applies. PHP.POS.LG.NGF.SOBTRAD.JSC.01-PUBLISHED 2024 P_240082_L 09.09.2024
 Plan 1 - 2000 Page 2 Page 4
Plan 1 - 2000 Page 2 Page 4