
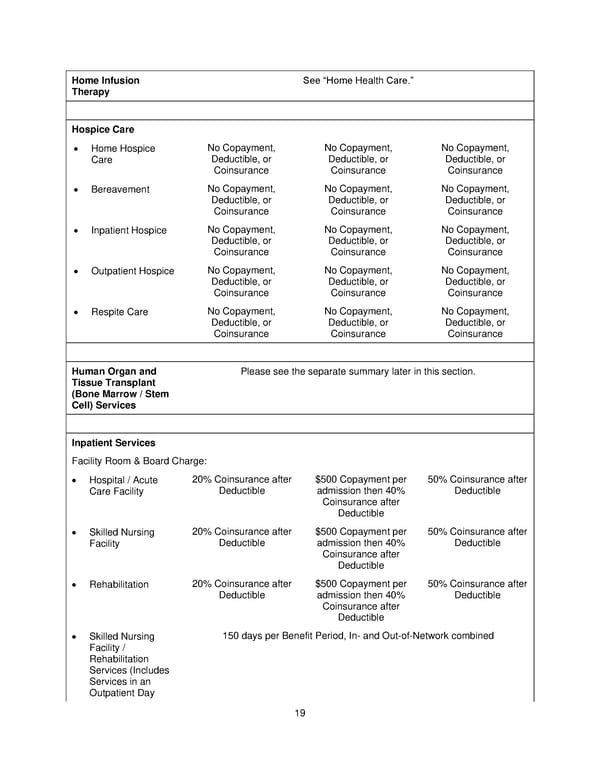
19 Home Infusion Therapy See Home Health Care. Hospice Care Home Hospice Care No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance Bereavement No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance Inpatient Hospice No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance Outpatient Hospice No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance Respite Care No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance Human Organ and Tissue Transplant (Bone Marrow / Stem Cell) Services Please see the separate summary later in this section. Inpatient Services Facility Room & Board Charge: Hospital / Acute Care Facility 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible Skilled Nursing Facility 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible Rehabilitation 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible Skilled Nursing Facility / Rehabilitation Services (Includes Services in an Outpatient Day 1 5 0 days per Benefit Period, In - and Out - of - Network combined
 Plan 1 SPD 2025 Page 19 Page 21
Plan 1 SPD 2025 Page 19 Page 21