
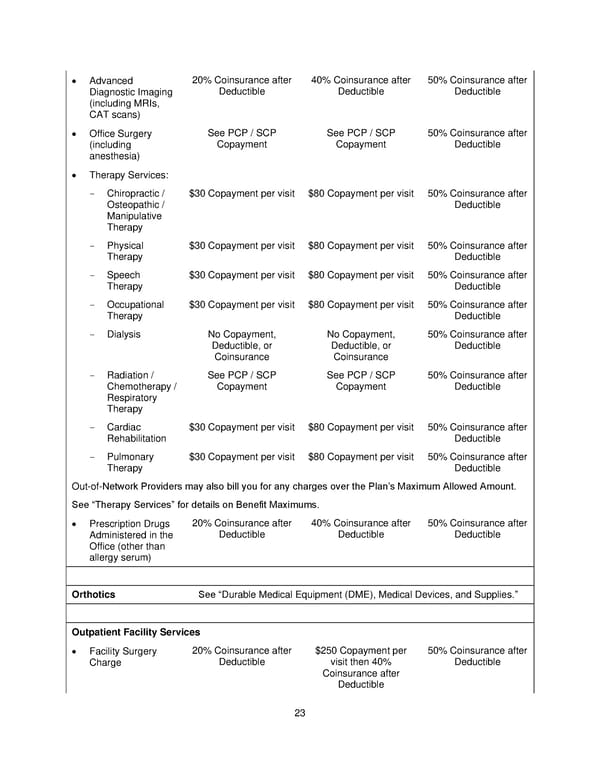
23 Advanced Diagnostic Imaging (including MRIs, CAT scans) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible Office Surgery (including anesthesia) See PCP / SCP Copayment See PCP / SCP Copayment 50% Coinsurance after Deductible Therapy Services: - Chiropractic / Osteopathic / Manipulative Therapy $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Deductible - Physical Therapy $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Deductible - Speech Therapy $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Deductible - Occupational Therapy $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Deductible - Dialysis No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible - Radiation / Chemotherapy / Respiratory Therapy See PCP / SCP Copayment See PCP / SCP Copayment 50% Coinsurance after Deductible - Cardiac Rehabilitation $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Deductible - Pulmonary Therapy $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Deductible Out - of - Network Providers may also bill you for any charges over the Plans Maximum Allowed Amount. See Therapy Services for details on Benefit Maximums. Prescription Drugs Administered in the Office (other than allergy serum) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible Orthotics See Durable Medical Equipment (DME), Medical Devices, and Supplies. Outpatient Facility Services Facility Surgery Charge 20% Coinsurance after Deductible $250 Copayment per visit then 40% Coinsurance after Deductible 50% Coinsurance after Deductible
 Plan 1 SPD 2025 Page 23 Page 25
Plan 1 SPD 2025 Page 23 Page 25