
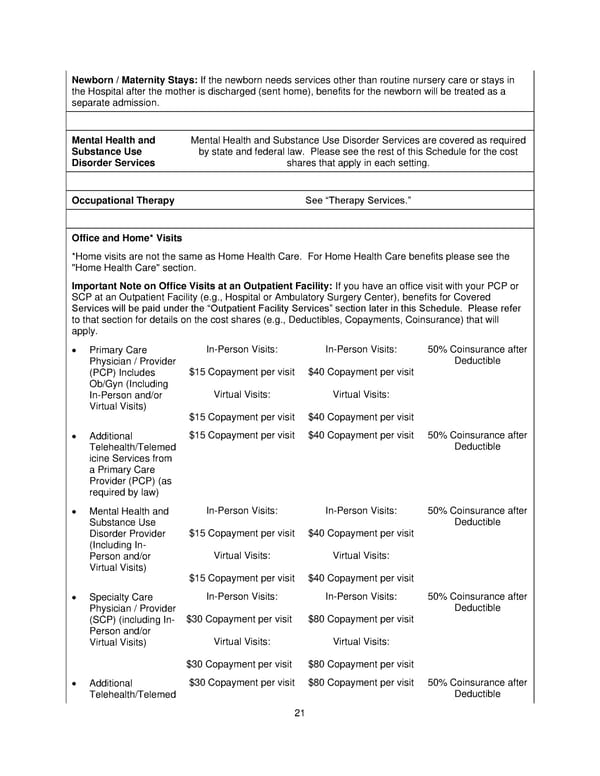
21 Newborn / Maternity Stays: If the newborn needs services other than routine nursery care or stays in the Hospital after the mother is discharged (sent home), benefits for the newborn will be treated as a separate admission. Mental Health and Substance Use Disorder Services Mental Health and Substance Use Disorder Services are covered as required by state and federal law. Please see the rest of this Schedule for the cost shares that apply in each setting. Occupational Therapy See Therapy Services. Office and Home* Visits *Home visits are not the same as Home Health Care. For Home Health Care benefits please see the "Home Health Care" section. Important Note on Office Visits at an Outpatient Facility: If you have an office visit with your PCP or SCP at an Outpatient Facility (e.g., Hospital or Ambulatory Su rgery Center ), benefits for Covered Services will be paid under the Outpatient Facility Services section later in this Schedule. Please refer to that section for details on the cost shares (e.g., Deductibles, Copayments, Coinsurance) that will apply. Primary Care Physician / Provider (PCP) Includes Ob/Gyn ( I ncluding In - Person and/or Virtual Visits) In - Person Visits: $15 Copayment per visit Virtual Visits: $15 Copayment per visit In - Person Visits: $40 Copayment per visit Virtual Visits: $40 Copayment per visit 50% Coinsurance after Deductible Additional Telehealth/Telemed icine Services from a Primary Care Provider (PCP) (as required by law) $15 Copayment per visit $40 Copayment per visit 50% Coinsurance after Deductible Mental Health and Substance Use Disorder Provider (Including In - Person and/or Virtual Visits) In - Person Visits: $15 Copayment per visit Virtual Visits: $15 Copayment per visit In - Person Visits: $40 Copayment per visit Virtual Visits: $40 Copayment per visit 50% Coinsurance after Deductible Specialty Care Physician / Provider (SCP) (including In - Person and/or Virtual Visits) In - Person Visits: $30 Copayment per visit Virtual Visits: $30 Copayment per visit In - Person Visits: $80 Copayment per visit Virtual Visits: $80 Copayment per visit 50% Coinsurance after Deductible Additional Telehealth/Telemed $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Deductible
 Plan 1 SPD 2025 Page 21 Page 23
Plan 1 SPD 2025 Page 21 Page 23