
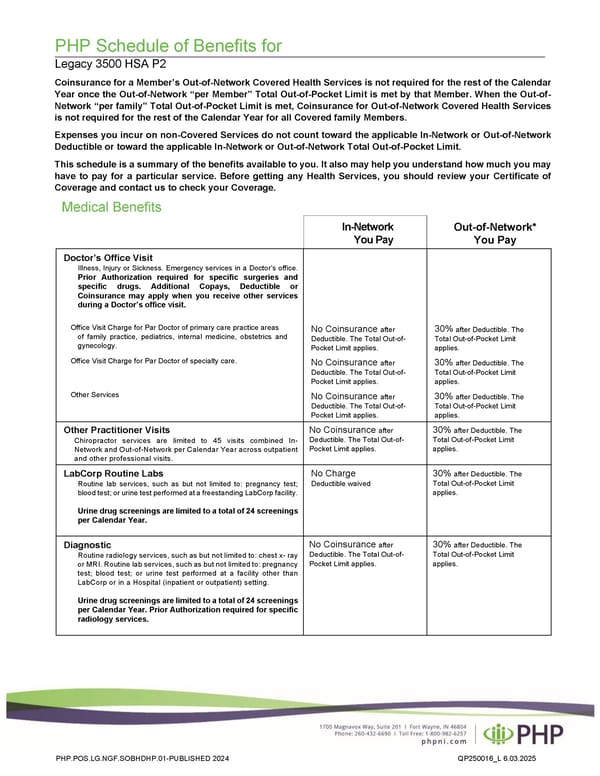
PHP Schedule of Benefits for Legacy 3500 HSA P2 Coinsurance for a Member’s Out-of-Network Covered Health Services is not required for the rest of the Calendar Year once the Out-of-Network “per Member” Total Out-of-Pocket Limit is met by that Member. When the Out-of- Network “per family” Total Out-of-Pocket Limit is met, Coinsurance for Out-of-Network Covered Health Services is not required for the rest of the Calendar Year for all Covered family Members. Expenses you incur on non-Covered Services do not count toward the applicable In-Network or Out-of-Network Deductible or toward the applicable In-Network or Out-of-Network Total Out-of-Pocket Limit. This schedule is a summary of the benefits available to you. It also may help you understand how much you may have to pay for a particular service. Before getting any Health Services, you should review your Certificate of Coverage and contact us to check your Coverage. Medical Benefits In-Network You Pay Doctor’s Office Visit Illness, Injury or Sickness. Emergency services in a Doctor’s office. Prior Authorization required for specific surgeries and specific drugs. Additional Copays, Deductible or Coinsurance may apply when you receive other services during a Doctor’s office visit. Office Visit Charge for Par Doctor of primary care practice areas of family practice, pediatrics, internal medicine, obstetrics and gynecology. Office Visit Charge for Par Doctor of specialty care. Other Services No Coinsurance after Deductible. The Total Out-of- Pocket Limit applies. No Coinsurance after Deductible. The Total Out-of- Pocket Limit applies. No Coinsurance after Deductible. The Total Out-of- Pocket Limit applies. 30% after Deductible. The Total Out-of-Pocket Limit applies. 30% after Deductible. The Total Out-of-Pocket Limit applies. 30% after Deductible. The Total Out-of-Pocket Limit applies. Other Practitioner Visits Chiropractor services are limited to 45 visits combined In- Network and Out-of-Network per Calendar Year across outpatient and other professional visits. No Coinsurance after Deductible. The Total Out-of- Pocket Limit applies. 30% after Deductible. The Total Out-of-Pocket Limit applies. LabCorp Routine Labs Routine lab services, such as but not limited to: pregnancy test; blood test; or urine test performed at a freestanding LabCorp facility. Urine drug screenings are limited to a total of 24 screenings per Calendar Year. No Charge Deductible waived 30% after Deductible. The Total Out-of-Pocket Limit applies. Diagnostic Routine radiology services, such as but not limited to: chest x- ray or MRI. Routine lab services, such as but not limited to: pregnancy test; blood test; or urine test performed at a facility other than LabCorp or in a Hospital (inpatient or outpatient) setting. Urine drug screenings are limited to a total of 24 screenings per Calendar Year. Prior Authorization required for specific radiology services. No Coinsurance after Deductible. The Total Out-of- Pocket Limit applies. 30% after Deductible. The Total Out-of-Pocket Limit applies. PHP.POS.LG.NGF.SOBHDHP.01-PUBLISHED 2024 QP250016_L 6.03.2025 Out-of-Network* You Pay
 Plan 2 - 3500 Page 1 Page 3
Plan 2 - 3500 Page 1 Page 3