
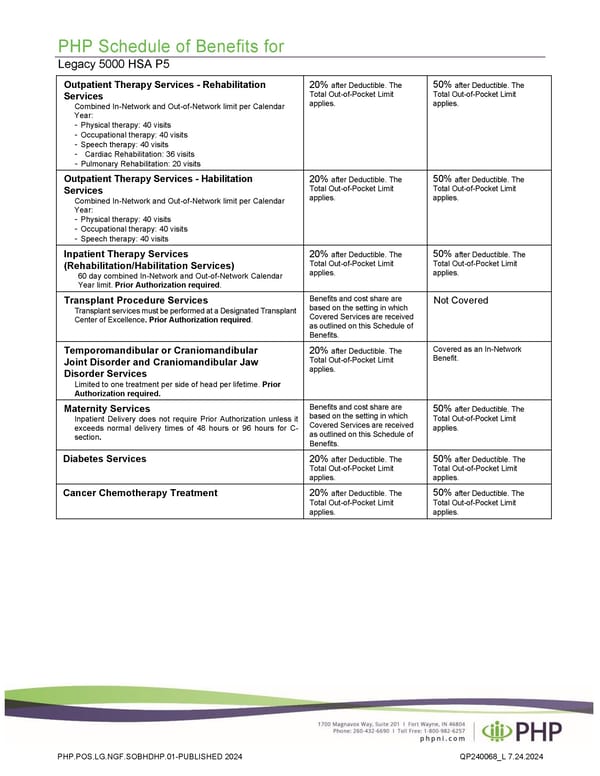
PHP Schedule of Benefits for Legacy 5000 HSA P5 Outpatient Therapy Services - Rehabilitation Services Combined In-Network and Out-of-Network limit per Calendar Year: - Physical therapy: 40 visits - Occupational therapy: 40 visits - Speech therapy: 40 visits - Cardiac Rehabilitation: 36 visits - Pulmonary Rehabilitation: 20 visits 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. Outpatient Therapy Services - Habilitation Services Combined In-Network and Out-of-Network limit per Calendar Year: - Physical therapy: 40 visits - Occupational therapy: 40 visits - Speech therapy: 40 visits 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. Inpatient Therapy Services (Rehabilitation/Habilitation Services) 60 day combined In-Network and Out-of-Network Calendar Year limit. Prior Authorization required. 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. Transplant Procedure Services Transplant services must be performed at a Designated Transplant Center of Excellence. Prior Authorization required. Benefits and cost share are based on the setting in which Covered Services are received as outlined on this Schedule of Benefits. Not Covered Temporomandibular or Craniomandibular Joint Disorder and Craniomandibular Jaw Disorder Services Limited to one treatment per side of head per lifetime. Prior Authorization required. 20% after Deductible. The Total Out-of-Pocket Limit applies. Covered as an In-Network Benefit. Maternity Services Inpatient Delivery does not require Prior Authorization unless it exceeds normal delivery times of 48 hours or 96 hours for C- section. Benefits and cost share are based on the setting in which Covered Services are received as outlined on this Schedule of Benefits. 50% after Deductible. The Total Out-of-Pocket Limit applies. Diabetes Services 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. Cancer Chemotherapy Treatment 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. PHP.POS.LG.NGF.SOBHDHP.01-PUBLISHED 2024 QP240068_L 7.24.2024
 Plan 3 - 6000 Page 3 Page 5
Plan 3 - 6000 Page 3 Page 5