
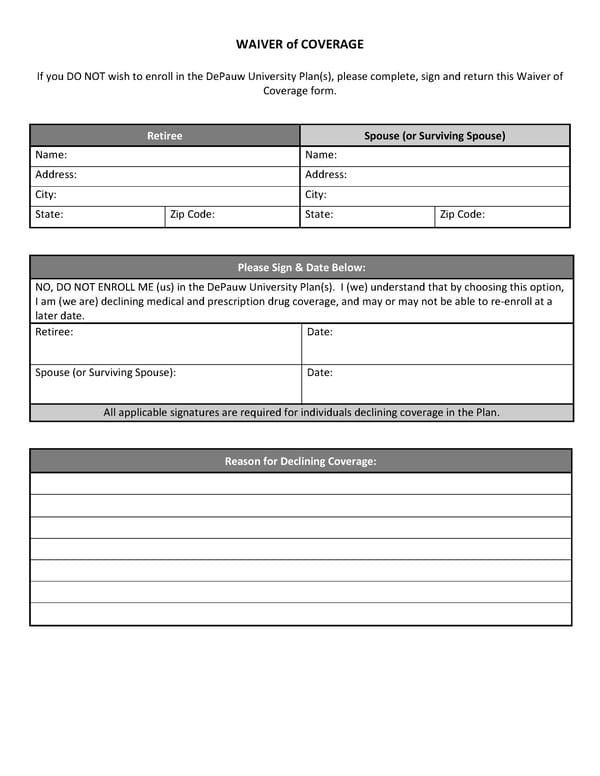
WAIVER of COVERAGE If you DO NOT wish to enroll in the DePauw University Plan(s), please complete, sign and return this Waiver of Coverage form. Retiree Spouse (or Surviving Spouse) Name: Name: Address: Address: City: City: State: Zip Code: State: Zip Code: Please Sign & Date Below: NO, DO NOT ENROLL ME (us) in the DePauw University Plan(s). I (we) understand that by choosing this option, I am (we are) declining medical and prescription drug coverage, and may or may not be able to re-enroll at a later date. Retiree: Date: Spouse (or Surviving Spouse): Date: All applicable signatures are required for individuals declining coverage in the Plan. Reason for Declining Coverage:
 Post-65 Retiree Guide_AmWins Page 22 Page 24
Post-65 Retiree Guide_AmWins Page 22 Page 24