
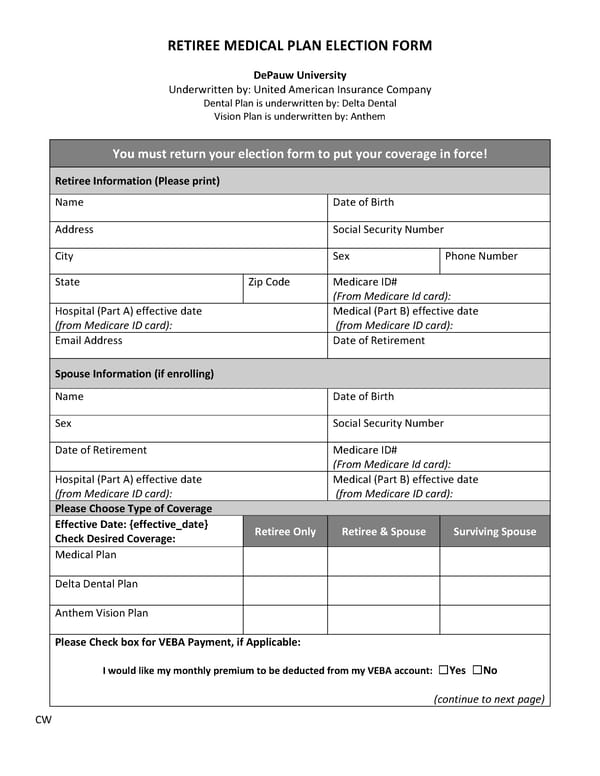
RETIREE MEDICAL PLAN ELECTION FORM DePauw University Underwritten by: United American Insurance Company Dental Plan is underwritten by: Delta Dental Vision Plan is underwritten by: Anthem You must return your election form to put your coverage in force! Retiree Information (Please print) Name Date of Birth Address Social Security Number City Sex Phone Number State Zip Code Medicare ID# (From Medicare Id card): Hospital (Part A) effective date Medical (Part B) effective date (from Medicare ID card): (from Medicare ID card): Email Address Date of Retirement Spouse Information (if enrolling) Name Date of Birth Sex Social Security Number Date of Retirement Medicare ID# (From Medicare Id card): Hospital (Part A) effective date Medical (Part B) effective date (from Medicare ID card): (from Medicare ID card): Please Choose Type of Coverage Effective Date: {effective_date} Retiree Only Retiree & Spouse Surviving Spouse Check Desired Coverage: Medical Plan Delta Dental Plan Anthem Vision Plan Please Check box for VEBA Payment, if Applicable: I would like my monthly premium to be deducted from my VEBA account: ☐Yes ☐No (continue to next page) CW
 Post-65 Retiree Guide_AmWins Page 14 Page 16
Post-65 Retiree Guide_AmWins Page 14 Page 16