
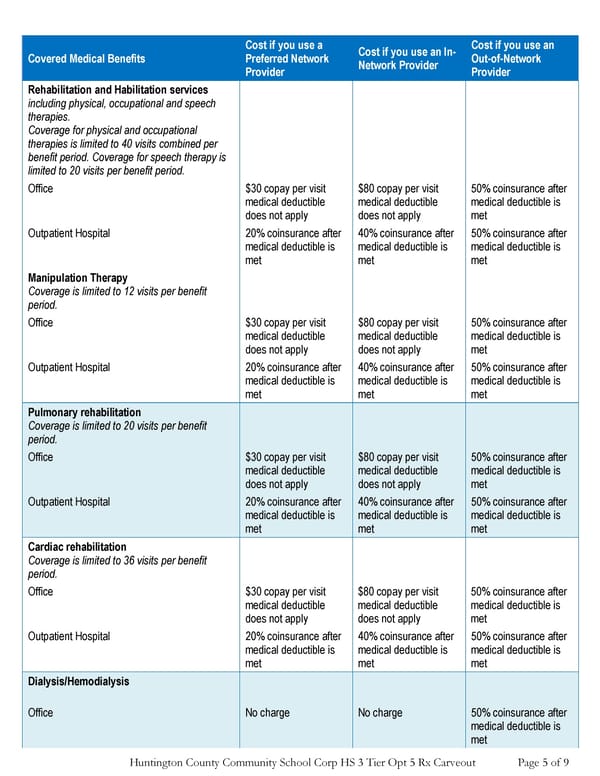
Huntington County Community School Corp HS 3 Tier Opt 5 Rx Carveout Page 5 of 9 Covered Medical Benefits Cost if you use a Preferred Network Provider Cost if you use an In- Network Provider Cost if you use an Out-of-Network Provider Rehabilitation and Habilitation services including physical, occupational and speech therapies. Coverage for physical and occupational therapies is limited to 40 visits combined per benefit period. Coverage for speech therapy is limited to 20 visits per benefit period. Office $30 copay per visit medical deductible does not apply $80 copay per visit medical deductible does not apply 50% coinsurance after medical deductible is met Outpatient Hospital 20% coinsurance after medical deductible is met 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Manipulation Therapy Coverage is limited to 12 visits per benefit period. Office $30 copay per visit medical deductible does not apply $80 copay per visit medical deductible does not apply 50% coinsurance after medical deductible is met Outpatient Hospital 20% coinsurance after medical deductible is met 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Pulmonary rehabilitation Coverage is limited to 20 visits per benefit period. Office $30 copay per visit medical deductible does not apply $80 copay per visit medical deductible does not apply 50% coinsurance after medical deductible is met Outpatient Hospital 20% coinsurance after medical deductible is met 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Cardiac rehabilitation Coverage is limited to 36 visits per benefit period. Office $30 copay per visit medical deductible does not apply $80 copay per visit medical deductible does not apply 50% coinsurance after medical deductible is met Outpatient Hospital 20% coinsurance after medical deductible is met 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Dialysis/Hemodialysis Office No charge No charge 50% coinsurance after medical deductible is met
 PPO #2 Summary Page 4 Page 6
PPO #2 Summary Page 4 Page 6