
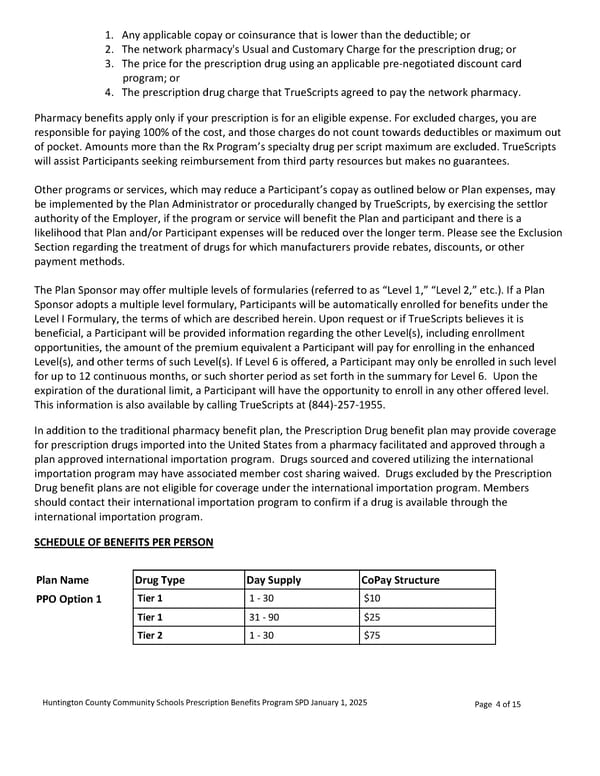
1. Any applicable copay or coinsurance that is lower than the deductible; or 2. The network pharmacy's Usual and Customary Charge for the prescription drug; or 3. The price for the prescription drug using an applicable pre-negotiated discount card program; or 4. The prescription drug charge that TrueScripts agreed to pay the network pharmacy. Pharmacy benefits apply only if your prescription is for an eligible expense. For excluded charges, you are responsible for paying 100% of the cost, and those charges do not count towards deductibles or maximum out of pocket. Amounts more than the Rx Program’s specialty drug per script maximum are excluded. TrueScripts will assist Participants seeking reimbursement from third party resources but makes no guarantees. Other programs or services, which may reduce a Participant’s copay as outlined below or Plan expenses, may be implemented by the Plan Administrator or procedurally changed by TrueScripts, by exercising the settlor authority of the Employer, if the program or service will benefit the Plan and participant and there is a likelihood that Plan and/or Participant expenses will be reduced over the longer term. Please see the Exclusion Section regarding the treatment of drugs for which manufacturers provide rebates, discounts, or other payment methods. The Plan Sponsor may offer multiple levels of formularies (referred to as “Level 1,” “Level 2,” etc.). If a Plan Sponsor adopts a multiple level formulary, Participants will be automatically enrolled for benefits under the Level I Formulary, the terms of which are described herein. Upon request or if TrueScripts believes it is beneficial, a Participant will be provided information regarding the other Level(s), including enrollment opportunities, the amount of the premium equivalent a Participant will pay for enrolling in the enhanced Level(s), and other terms of such Level(s). If Level 6 is offered, a Participant may only be enrolled in such level for up to 12 continuous months, or such shorter period as set forth in the summary for Level 6. Upon the expiration of the durational limit, a Participant will have the opportunity to enroll in any other offered level. This information is also available by calling TrueScripts at (844)-257-1955. In addition to the traditional pharmacy benefit plan, the Prescription Drug benefit plan may provide coverage for prescription drugs imported into the United States from a pharmacy facilitated and approved through a plan approved international importation program. Drugs sourced and covered utilizing the international importation program may have associated member cost sharing waived. Drugs excluded by the Prescription Drug benefit plans are not eligible for coverage under the international importation program. Members should contact their international importation program to confirm if a drug is available through the international importation program. SCHEDULE OF BENEFITS PER PERSON Plan Name Drug Type Day Supply CoPay Structure PPO Option 1 Tier 1 1 - 30 $10 Tier 1 31 - 90 $25 Tier 2 1 - 30 $75 Huntington County Community Schools Prescription Benefits Program SPD January 1, 2025 Page 4 of 15
 Prescription Summary Plan Description Page 3 Page 5
Prescription Summary Plan Description Page 3 Page 5