
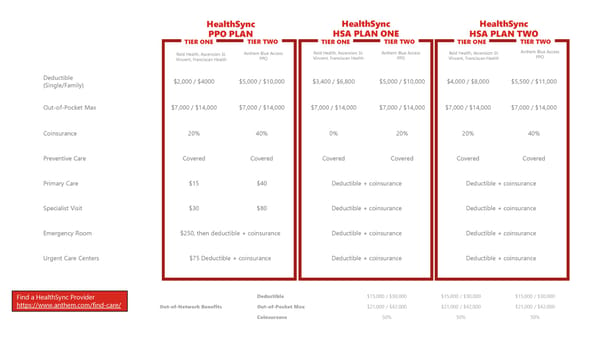
Deductible (Single/Family) $2,000 / $4000 $5,000 / $10,000 $3,400 / $6,800 $5,000 / $10,000 $4,000 / $8,000 $5,500 / $11,000 Out-of-Pocket Max $7,000 / $14,000 $7,000 / $14,000 $7,000 / $14,000 $7,000 / $14,000 $7,000 / $14,000 $7,000 / $14,000 Coinsurance 20% 40% 0% 20% 20% 40% Preventive Care Covered Covered Covered Covered Covered Covered Primary Care $15 $40 Deductible + coinsurance Deductible + coinsurance Specialist Visit $30 $80 Deductible + coinsurance Deductible + coinsurance Emergency Room $250, then deductible + coinsurance Deductible + coinsurance Deductible + coinsurance Urgent Care Centers $75 Deductible + coinsurance Deductible + coinsurance Deductible + coinsurance HealthSync PPO PLAN TIER ONE TIER TWO HealthSync HSA PLAN ONE TIER ONE TIER TWO HealthSync HSA PLAN TWO TIER ONE TIER TWO Out-of-Network Benefits Deductible $15,000 / $30,000 $15,000 / $30,000 $15,000 / $30,000 Out-of-Pocket Max $21,000 / $42,000 $21,000 / $42,000 $21,000 / $42,000 Coinsurance 50% 50% 50% Reid Health, Ascension St. Vincent, Franciscan Health Anthem Blue Access PPO Anthem Blue Access PPO Anthem Blue Access PPO Reid Health, Ascension St. Vincent, Franciscan Health Reid Health, Ascension St. Vincent, Franciscan Health Find a HealthSync Provider https://www.anthem.com/find-care/
 Richmond Community Schools Employee Benefits Page 7 Page 9
Richmond Community Schools Employee Benefits Page 7 Page 9