
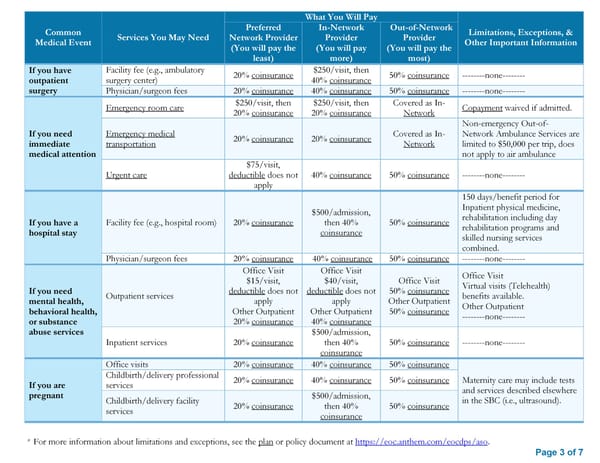
* For more information about limitations and exceptions, see the plan or policy document at https://eoc.anthem.com/eocdps/aso. Page 3 of 7 Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information Preferred Network Provider (You will pay the least) In-Network Provider (You will pay more) Out-of-Network Provider (You will pay the most) If you have outpatient surgery Facility fee (e.g., ambulatory surgery center) 20% coinsurance $250/visit, then 40% coinsurance 50% coinsurance --------none-------- Physician/surgeon fees 20% coinsurance 40% coinsurance 50% coinsurance --------none-------- If you need immediate medical attention Emergency room care $250/visit, then 20% coinsurance $250/visit, then 20% coinsurance Covered as In- Network Copayment waived if admitted. Emergency medical transportation 20% coinsurance 20% coinsurance Covered as In- Network Non-emergency Out-of- Network Ambulance Services are limited to $50,000 per trip, does not apply to air ambulance Urgent care $75/visit, deductible does not apply 40% coinsurance 50% coinsurance --------none-------- If you have a hospital stay Facility fee (e.g., hospital room) 20% coinsurance $500/admission, then 40% coinsurance 50% coinsurance 150 days/benefit period for Inpatient physical medicine, rehabilitation including day rehabilitation programs and skilled nursing services combined. Physician/surgeon fees 20% coinsurance 40% coinsurance 50% coinsurance --------none-------- If you need mental health, behavioral health, or substance abuse services Outpatient services Office Visit $15/visit, deductible does not apply Other Outpatient 20% coinsurance Office Visit $40/visit, deductible does not apply Other Outpatient 40% coinsurance Office Visit 50% coinsurance Other Outpatient 50% coinsurance Office Visit Virtual visits (Telehealth) benefits available. Other Outpatient --------none-------- Inpatient services 20% coinsurance $500/admission, then 40% coinsurance 50% coinsurance --------none-------- If you are pregnant Office visits 20% coinsurance 40% coinsurance 50% coinsurance Maternity care may include tests and services described elsewhere in the SBC (i.e., ultrasound). Childbirth/delivery professional services 20% coinsurance 40% coinsurance 50% coinsurance Childbirth/delivery facility services 20% coinsurance $500/admission, then 40% coinsurance 50% coinsurance
 SBC: Plan 2 Page 2 Page 4
SBC: Plan 2 Page 2 Page 4