
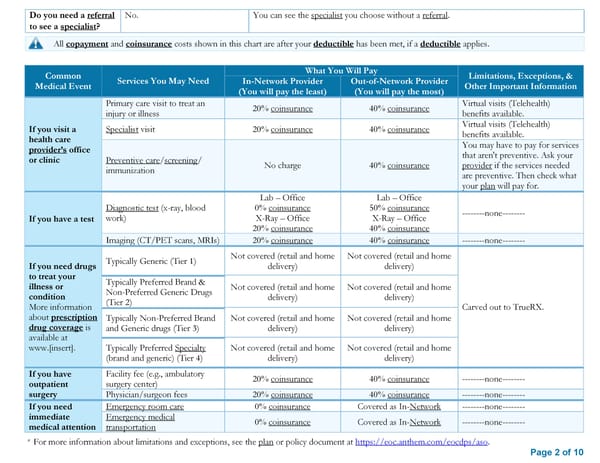
Do you need a referral No. You can see the specialist you choose without a referral. to see a specialist? All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies. Common What You Will Pay Limitations, Exceptions, & Medical Event Services You May Need In-Network Provider Out-of-Network Provider Other Important Information (You will pay the least) (You will pay the most) Primary care visit to treat an 20% coinsurance 40% coinsurance Virtual visits (Telehealth) injury or illness benefits available. If you visit a Specialist visit 20% coinsurance 40% coinsurance Virtual visits (Telehealth) health care benefits available. provider’s office You may have to pay for services or clinic Preventive care/screening/ that aren't preventive. Ask your immunization No charge 40% coinsurance provider if the services needed are preventive. Then check what your plan will pay for. Lab – Office Lab – Office Diagnostic test (x-ray, blood 0% coinsurance 50% coinsurance --------none-------- If you have a test work) X-Ray – Office X-Ray – Office 20% coinsurance 40% coinsurance Imaging (CT/PET scans, MRIs) 20% coinsurance 40% coinsurance --------none-------- Typically Generic (Tier 1) Not covered (retail and home Not covered (retail and home If you need drugs delivery) delivery) to treat your Typically Preferred Brand & illness or Non-Preferred Generic Drugs Not covered (retail and home Not covered (retail and home condition (Tier 2) delivery) delivery) More information Carved out to TrueRX. about prescription Typically Non-Preferred Brand Not covered (retail and home Not covered (retail and home drug coverage is and Generic drugs (Tier 3) delivery) delivery) available at www.[insert]. Typically Preferred Specialty Not covered (retail and home Not covered (retail and home (brand and generic) (Tier 4) delivery) delivery) If you have Facility fee (e.g., ambulatory 20% coinsurance 40% coinsurance --------none-------- outpatient surgery center) surgery Physician/surgeon fees 20% coinsurance 40% coinsurance --------none-------- If you need Emergency room care 0% coinsurance Covered as In-Network --------none-------- immediate Emergency medical 0% coinsurance Covered as In-Network --------none-------- medical attention transportation * For more information about limitations and exceptions, see the plan or policy document at https://eoc.anthem.com/eocdps/aso. Page 2 of 10
 Summary of Benefits and Coverage: Anthem Blue Access PPO HSA Page 1 Page 3
Summary of Benefits and Coverage: Anthem Blue Access PPO HSA Page 1 Page 3