
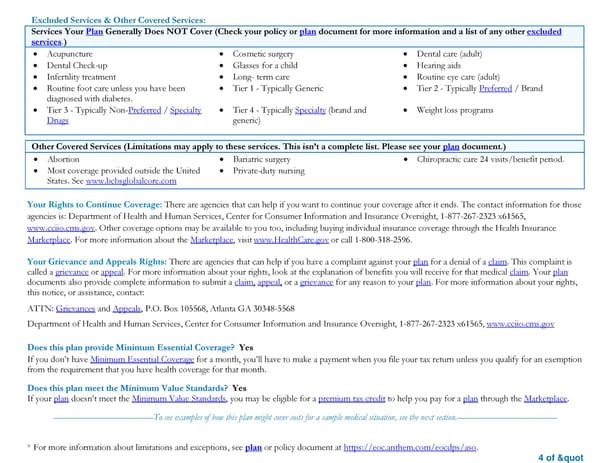
* For more information about limitations and exceptions, see plan or policy document at https://eoc.anthem.com/eocdps/aso. 4 of " Excluded Services & Other Covered Services: Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.) • Acupuncture • Cosmetic surgery • Dental care (adult) • Dental Check-up • Glasses for a child • Hearing aids • Infertility treatment • Long- term care • Routine eye care (adult) • Routine foot care unless you have been diagnosed with diabetes. • Tier 1 - Typically Generic • Tier 2 - Typically Preferred / Brand • Tier 3 - Typically Non-Preferred / Specialty Drugs • Tier 4 - Typically Specialty (brand and generic) • Weight loss programs Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.) • Abortion • Bariatric surgery • Chiropractic care 24 visits/benefit period. • Most coverage provided outside the United States. See www.bcbsglobalcore.com • Private-duty nursing Your Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: Department of Health and Human Services, Center for Consumer Information and Insurance Oversight, 1-877-267-2323 x61565, www.cciio.cms.gov. Other coverage options may be available to you too, including buying individual insurance coverage through the Health Insurance Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596. Your Grievance and Appeals Rights: There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance, contact: ATTN: Grievances and Appeals, P.O. Box 105568, Atlanta GA 30348-5568 Department of Health and Human Services, Center for Consumer Information and Insurance Oversight, 1-877-267-2323 x61565, www.cciio.cms.gov Does this plan provide Minimum Essential Coverage? Yes If you don’t have Minimum Essential Coverage for a month, you’ll have to make a payment when you file your tax return unless you qualify for an exemption from the requirement that you have health coverage for that month. Does this plan meet the Minimum Value Standards? Yes If your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace. ––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next section.––––––––––––––––––––––
 Summary of Benefits and Coverage - Ball State University PPO Health Plan Page 3 Page 5
Summary of Benefits and Coverage - Ball State University PPO Health Plan Page 3 Page 5