
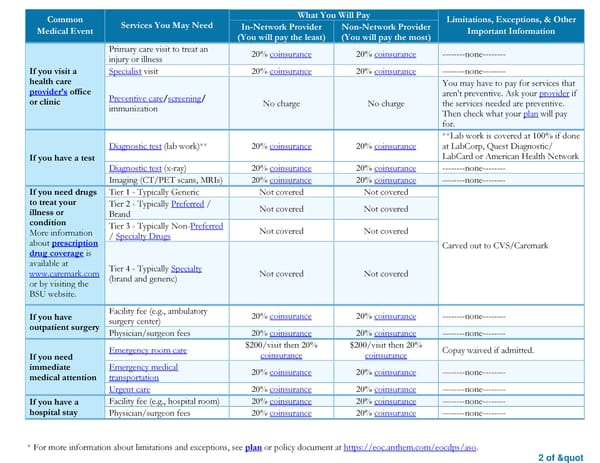
* For more information about limitations and exceptions, see plan or policy document at https://eoc.anthem.com/eocdps/aso. 2 of " Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information In-Network Provider (You will pay the least) Non-Network Provider (You will pay the most) If you visit a health care provider’s office or clinic Primary care visit to treat an injury or illness 20% coinsurance 20% coinsurance --------none-------- Specialist visit 20% coinsurance 20% coinsurance --------none-------- Preventive care/screening/ immunization No charge No charge You may have to pay for services that aren't preventive. Ask your provider if the services needed are preventive. Then check what your plan will pay for. If you have a test Diagnostic test (lab work)** 20% coinsurance 20% coinsurance **Lab work is covered at 100% if done at LabCorp, Quest Diagnostic/ LabCard or American Health Network Diagnostic test (x-ray) 20% coinsurance 20% coinsurance --------none-------- Imaging (CT/PET scans, MRIs) 20% coinsurance 20% coinsurance --------none-------- If you need drugs to treat your illness or condition More information about prescription drug coverage is available at www.caremark.com or by visiting the BSU website. Tier 1 - Typically Generic Not covered Not covered Carved out to CVS/Caremark Tier 2 - Typically Preferred / Brand Not covered Not covered Tier 3 - Typically Non-Preferred / Specialty Drugs Not covered Not covered Tier 4 - Typically Specialty (brand and generic) Not covered Not covered If you have outpatient surgery Facility fee (e.g., ambulatory surgery center) 20% coinsurance 20% coinsurance --------none-------- Physician/surgeon fees 20% coinsurance 20% coinsurance --------none-------- If you need immediate medical attention Emergency room care $200/visit then 20% coinsurance $200/visit then 20% coinsurance Copay waived if admitted. Emergency medical transportation 20% coinsurance 20% coinsurance --------none-------- Urgent care 20% coinsurance 20% coinsurance --------none-------- If you have a hospital stay Facility fee (e.g., hospital room) 20% coinsurance 20% coinsurance --------none-------- Physician/surgeon fees 20% coinsurance 20% coinsurance --------none--------
 Summary of Benefits and Coverage: Retiree Over Age 65/Medicare Disabled Non EGWP Health Plan CMM Page 1 Page 3
Summary of Benefits and Coverage: Retiree Over Age 65/Medicare Disabled Non EGWP Health Plan CMM Page 1 Page 3