
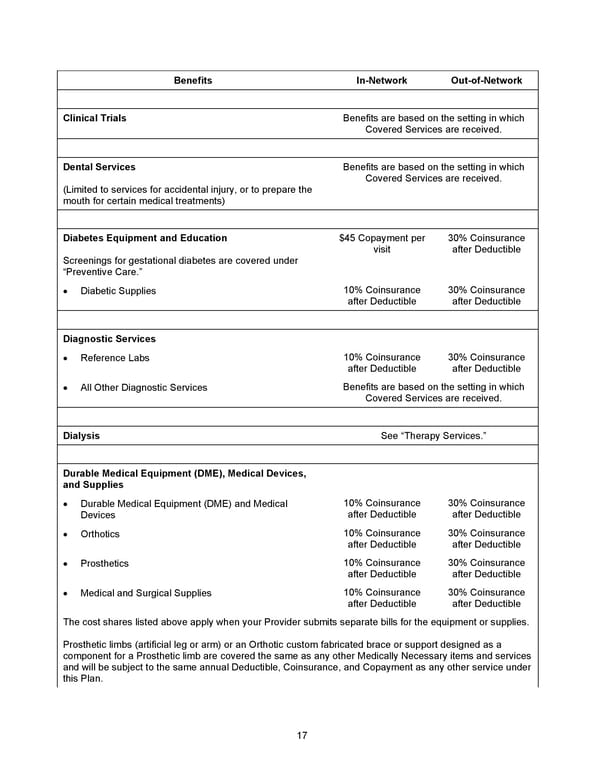
17 Benefits In - Network Out - of - Network Clinical Trials Benefits are based on the setting in which Covered Services are received. Dental Services (Limited to services for accidental injury, or to prepare the mouth for certain medical treatments) Benefits are based on the setting in which Covered Services are received. Diabetes Equipment and Education Screenings for gestational diabetes are covered under “Preventive Care. ” $45 Copayment per visit 30% Coinsurance after Deductible • Diabetic Supplies 10% Coinsurance after Deductible 30% Coinsurance after Deductible Diagnostic Services • Reference Labs 10% Coinsurance after Deductible 30% Coinsurance after Deductible • All Other Diagnostic Services Benefits are based on the setting in which Covered Services are received. Dialysis See “Therapy Services.” Durable Medical Equipment (DME), Medical Devices, and Supplies • Durable Medical Equipment (DME) and Medical Devices 10% Coinsurance after Deductible 30% Coinsurance after Deductible • Orthotics 10% Coinsurance after Deductible 30% Coinsurance after Deductible • Prosthetics 10% Coinsurance after Deductible 30% Coinsurance after Deductible • Medical and Surgical Supplies 10% Coinsurance after Deductible 30% Coinsurance after Deductible The cost shares listed above apply when your Provider submits separate bills for the equipment or supplies. Prosthetic limbs (artificial leg or arm) or an Orthotic custom fabricated brace or support designed as a component for a Prosthetic limb are covered the same as any other Medically Necessary items and services and will be subject to the same annual Deductible, Coinsurance, and Copayment as any other service under this Plan.
 2026 Anthem Certificate Plan A Page 17 Page 19
2026 Anthem Certificate Plan A Page 17 Page 19