
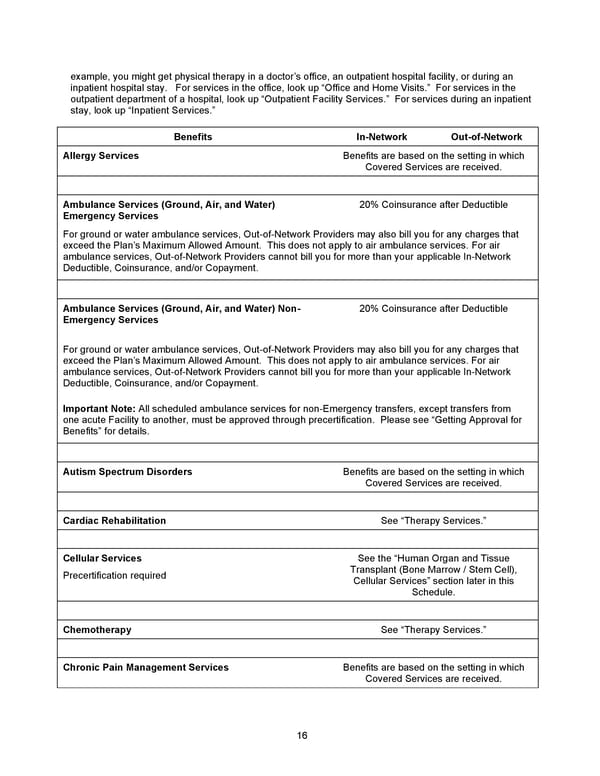
16 example, you might get physical therapy in a doctor’s office, an outpatient hospital facility, or during an inpatient hospital stay. For services in the office, look up “Office and Home Visits.” For services in the outpatient department of a hospital, l ook up “Outpatient Facility Services.” For services during an inpatient stay, look up “Inpatient Services.” Benefits In - Network Out - of - Network Allergy Services Benefits are based on the setting in which Covered Services are received. Ambulance Services (Ground, Air, and Water) Emergency Services 2 0% Coinsurance after Deductible For ground or water ambulance services, Out - of - Network Providers may also bill you for any charges that exceed the Plan’s Maximum Allowed Amount. This does not apply to air ambulance services. For air ambulance services, Out - of - Network Providers cannot bill you for more than your applicable In - Network Deductible, Coinsurance, and/or Copayment . Ambulance Services (Ground, Air, and Water) Non - Emergency Services 2 0% Coinsurance after Deductible For ground or water ambulance services, Out - of - Network Providers may also bill you for any charges that exceed the Plan’s Maximum Allowed Amount. This does not apply to air ambulance services. For air ambulance services, Out - of - Network Providers cannot bi ll you for more than your applicable In - Network Deductible, Coinsurance, and/or Copayment . Important Note: All scheduled ambulance services for non - Emergency transfers, except transfers from one acute Facility to another, must be approved through precertification. Please see “Getting Approval for Benefits” for details. Autism Spectrum Disorders Benefits are based on the setting in which Covered Services are received. Cardiac Rehabilitation See “Therapy Services.” Cellular Services Precertification required See the “Human Organ and Tissue Transplant (Bone Marrow / Stem Cell), Cellular Services” section later in this Schedule. Chemotherapy See “Therapy Services.” Chronic Pain Management Services Benefits are based on the setting in which Covered Services are received.
 2026 Anthem Certificate Plan A Page 16 Page 18
2026 Anthem Certificate Plan A Page 16 Page 18