
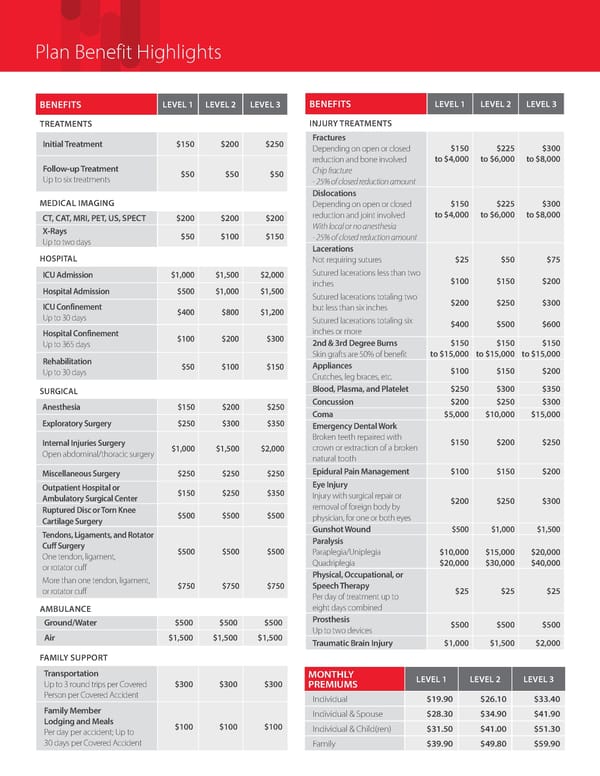
Plan Benefit Highlights ALL COVERAGE LEVELS BENEFITS LEVEL 1 LEVEL 2 LEVEL 3 BENEFITS LEVEL 1 LEVEL 2 LEVEL 3 TREATMENTS INJURY TREATMENTS ALL COVERAGE Initial Treatment $150 $200 $250 Fractures LEVELS Depending on open or closed $150 $225 $300 reduction and bone involved to $4,000 to $6,000 to $8,000 Follow-up Treatment $50 $50 $50 Chip fracture Up to six treatments - 25% of closed reduction amount Dislocations MEDICAL IMAGING Depending on open or closed $150 $225 $300 CT, CAT, MRI, PET, US, SPECT $200 $200 $200 reduction and joint involved to $4,000 to $6,000 to $8,000 X-Rays With local or no anesthesia Up to two days $50 $100 $150 - 25% of closed reduction amount Lacerations HOSPITAL Not requiring sutures $25 $50 $75 ICU Admission $1,000 $1,500 $2,000 Sutured lacerations less than two inches $100 $150 $200 Hospital Admission $500 $1,000 $1,500 Sutured lacerations totaling two ICU Confinement but less than six inches $200 $250 $300 Up to 30 days $400 $800 $1,200 Sutured lacerations totaling six $400 $500 $600 Hospital Confinement $100 $200 $300 inches or more Up to 365 days 2nd & 3rd Degree Burns $150 $150 $150 Rehabilitation Skin grafts are 50% of benefit to $15,000 to $15,000 to $15,000 Up to 30 days $50 $100 $150 Appliances $100 $150 $200 Crutches, leg braces, etc. SURGICAL Blood, Plasma, and Platelet $250 $300 $350 Anesthesia $150 $200 $250 Concussion $200 $250 $300 Coma $5,000 $10,000 $15,000 Exploratory Surgery $250 $300 $350 Emergency Dental Work Internal Injuries Surgery Broken teeth repaired with $150 $200 $250 Open abdominal/thoracic surgery $1,000 $1,500 $2,000 crown or extraction of a broken natural tooth Miscellaneous Surgery $250 $250 $250 Epidural Pain Management $100 $150 $200 Outpatient Hospital or Eye Injury Ambulatory Surgical Center $150 $250 $350 Injury with surgical repair or removal of foreign body by $200 $250 $300 Ruptured Disc or Torn Knee $500 $500 $500 physician, for one or both eyes Cartilage Surgery Gunshot Wound $500 $1,000 $1,500 Tendons, Ligaments, and Rotator Paralysis Cuff Surgery $500 $500 $500 Paraplegia/Uniplegia $10,000 $15,000 $20,000 One tendon, ligament, Quadriplegia $20,000 $30,000 $40,000 or rotator cuff Physical, Occupational, or More than one tendon, ligament, $750 $750 $750 Speech Therapy or rotator cuff Per day of treatment up to $25 $25 $25 AMBULANCE eight days combined Ground/Water $500 $500 $500 Prosthesis $500 $500 $500 Air $1,500 $1,500 $1,500 Up to two devices Traumatic Brain Injury $1,000 $1,500 $2,000 FAMILY SUPPORT Transportation MONTHLY LEVEL 1 LEVEL 2 LEVEL 3 Up to 3 round trips per Covered $300 $300 $300 PREMIUMS Person per Covered Accident Individual $19.90 $26.10 $33.40 Family Member Individual & Spouse $28.30 $34.90 $41.90 Lodging and Meals $100 $100 $100 Individual & Child(ren) $31.50 $41.00 $51.30 Per day per accident; Up to 30 days per Covered Accident Family $39.90 $49.80 $59.90
 Accident (New Brochure) Page 1 Page 3
Accident (New Brochure) Page 1 Page 3