
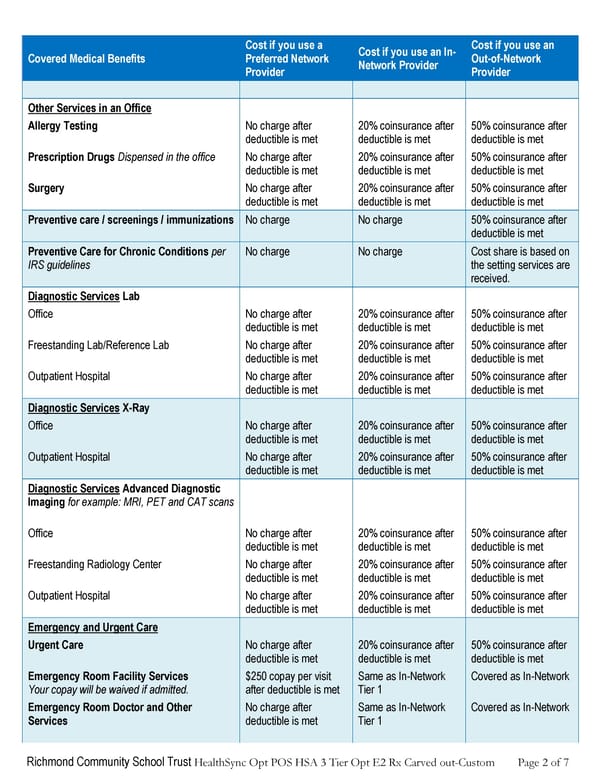
Richmond Community School Trust HealthSync Opt POS HSA 3 Tier Opt E2 Rx Carved out-Custom Page 2 of 7 Covered Medical Benefits Cost if you use a Preferred Network Provider Cost if you use an In- Network Provider Cost if you use an Out-of-Network Provider Other Services in an Office Allergy Testing No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Prescription Drugs Dispensed in the office No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Surgery No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Preventive care / screenings / immunizations No charge No charge 50% coinsurance after deductible is met Preventive Care for Chronic Conditions per IRS guidelines No charge No charge Cost share is based on the setting services are received. Diagnostic Services Lab Office No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Freestanding Lab/Reference Lab No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Outpatient Hospital No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Diagnostic Services X-Ray Office No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Outpatient Hospital No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Diagnostic Services Advanced Diagnostic Imaging for example: MRI, PET and CAT scans Office No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Freestanding Radiology Center No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Outpatient Hospital No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Emergency and Urgent Care Urgent Care No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Emergency Room Facility Services Your copay will be waived if admitted. $250 copay per visit after deductible is met Same as In-Network Tier 1 Covered as In-Network Emergency Room Doctor and Other Services No charge after deductible is met Same as In-Network Tier 1 Covered as In-Network
 Anthem Summary of Benefits HDHP #1 Page 1 Page 3
Anthem Summary of Benefits HDHP #1 Page 1 Page 3