
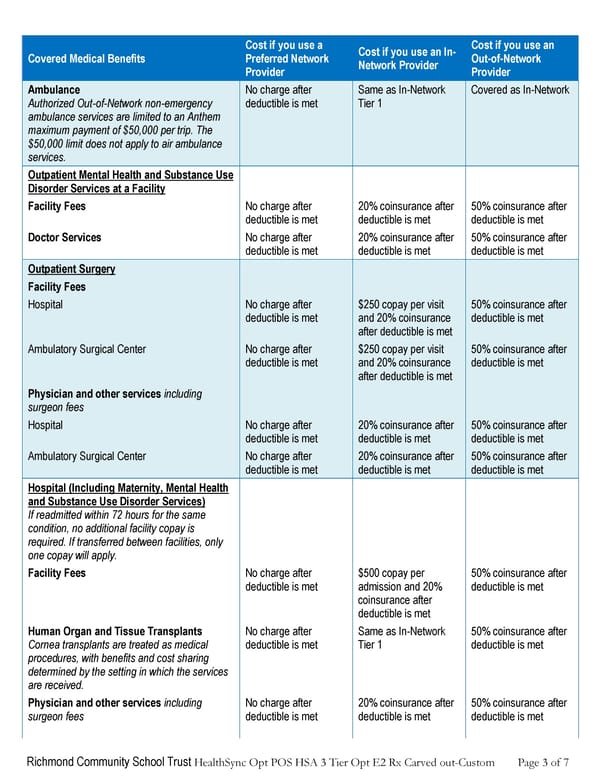
Richmond Community School Trust HealthSync Opt POS HSA 3 Tier Opt E2 Rx Carved out-Custom Page 3 of 7 Covered Medical Benefits Cost if you use a Preferred Network Provider Cost if you use an In- Network Provider Cost if you use an Out-of-Network Provider Ambulance Authorized Out-of-Network non-emergency ambulance services are limited to an Anthem maximum payment of $50,000 per trip. The $50,000 limit does not apply to air ambulance services. No charge after deductible is met Same as In-Network Tier 1 Covered as In-Network Outpatient Mental Health and Substance Use Disorder Services at a Facility Facility Fees No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Doctor Services No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Outpatient Surgery Facility Fees Hospital No charge after deductible is met $250 copay per visit and 20% coinsurance after deductible is met 50% coinsurance after deductible is met Ambulatory Surgical Center No charge after deductible is met $250 copay per visit and 20% coinsurance after deductible is met 50% coinsurance after deductible is met Physician and other services including surgeon fees Hospital No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Ambulatory Surgical Center No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met Hospital (Including Maternity, Mental Health and Substance Use Disorder Services) If readmitted within 72 hours for the same condition, no additional facility copay is required. If transferred between facilities, only one copay will apply. Facility Fees No charge after deductible is met $500 copay per admission and 20% coinsurance after deductible is met 50% coinsurance after deductible is met Human Organ and Tissue Transplants Cornea transplants are treated as medical procedures, with benefits and cost sharing determined by the setting in which the services are received. No charge after deductible is met Same as In-Network Tier 1 50% coinsurance after deductible is met Physician and other services including surgeon fees No charge after deductible is met 20% coinsurance after deductible is met 50% coinsurance after deductible is met
 Anthem Summary of Benefits HDHP #1 Page 2 Page 4
Anthem Summary of Benefits HDHP #1 Page 2 Page 4