
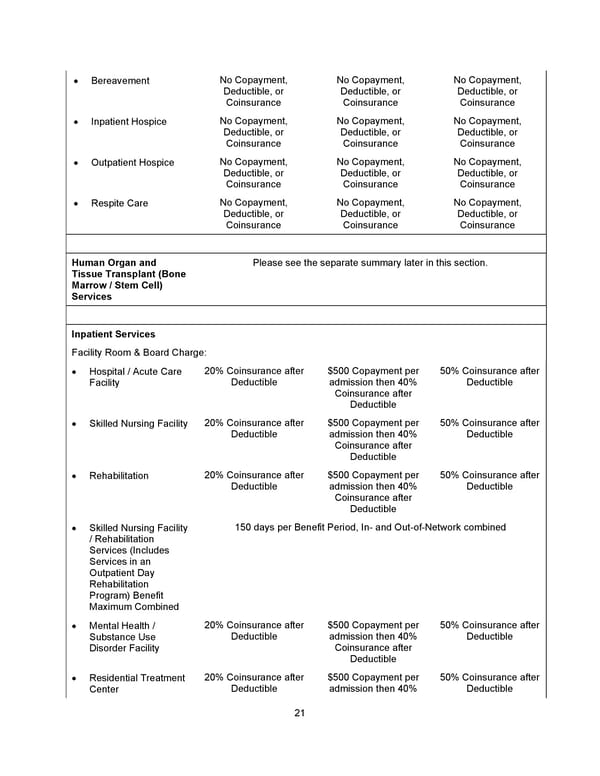
21 • Bereavement No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance • Inpatient Hospice No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance • Outpatient Hospice No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance • Respite Care No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance Human Organ and Tissue Transplant (Bone Marrow / Stem Cell) Services Please see the separate summary later in this section. Inpatient Services Facility Room & Board Charge: • Hospital / Acute Care Facility 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Skilled Nursing Facility 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Rehabilitation 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Skilled Nursing Facility / Rehabilitation Services (Includes Services in an Outpatient Day Rehabilitation Program) Benefit Maximum Combined 150 days per Benefit Period, In- and Out-of-Network combined • Mental Health / Substance Use Disorder Facility 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Residential Treatment Center 20% Coinsurance after Deductible $500 Copayment per admission then 40% 50% Coinsurance after Deductible
 Benefit Booklet: Plan 2 Page 21 Page 23
Benefit Booklet: Plan 2 Page 21 Page 23