
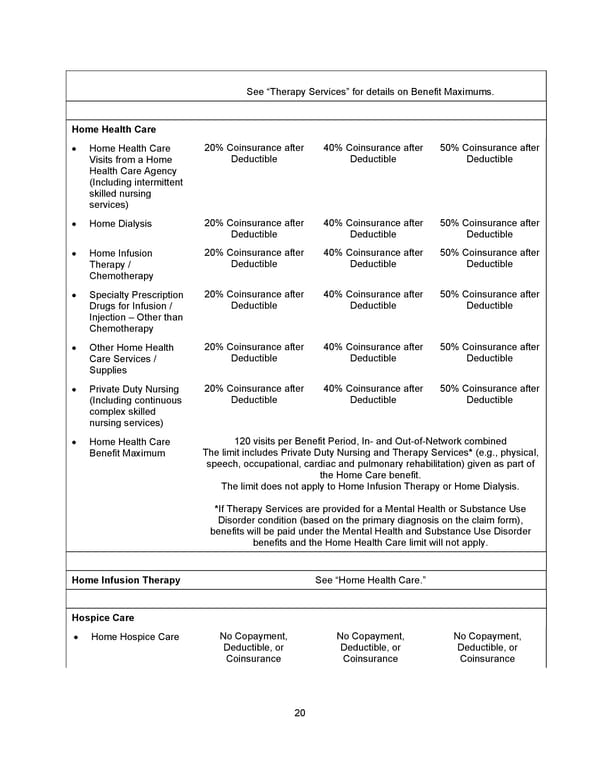
20 See “Therapy Services” for details on Benefit Maximums. Home Health Care • Home Health Care Visits from a Home Health Care Agency (Including intermittent skilled nursing services) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Home Dialysis 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Home Infusion Therapy / Chemotherapy 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Specialty Prescription Drugs for Infusion / Injection – Other than Chemotherapy 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Other Home Health Care Services / Supplies 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Private Duty Nursing (Including continuous complex skilled nursing services) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Home Health Care Benefit Maximum 120 visits per Benefit Period, In- and Out-of-Network combined The limit includes Private Duty Nursing and Therapy Services* (e.g., physical, speech, occupational, cardiac and pulmonary rehabilitation) given as part of the Home Care benefit. The limit does not apply to Home Infusion Therapy or Home Dialysis. *If Therapy Services are provided for a Mental Health or Substance Use Disorder condition (based on the primary diagnosis on the claim form), benefits will be paid under the Mental Health and Substance Use Disorder benefits and the Home Health Care limit will not apply. Home Infusion Therapy See “Home Health Care.” Hospice Care • Home Hospice Care No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance
 Benefit Booklet: Plan 2 Page 20 Page 22
Benefit Booklet: Plan 2 Page 20 Page 22