
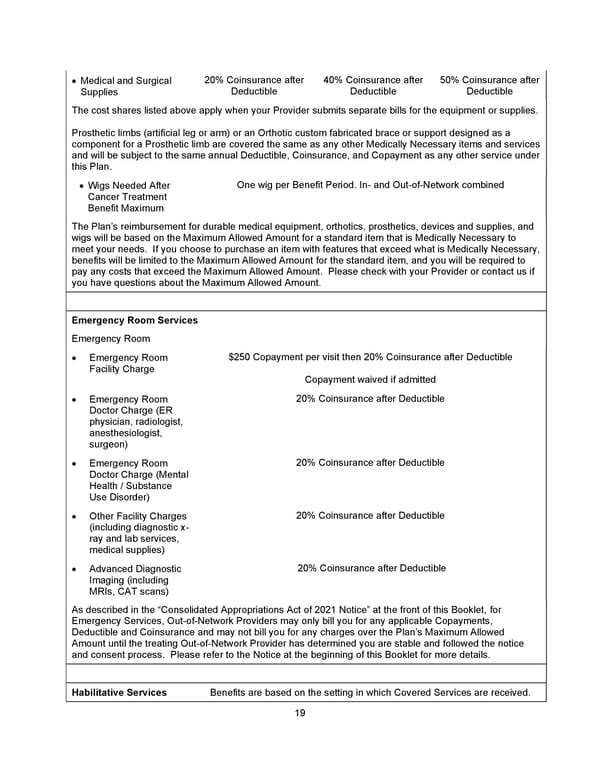
19 • Medical and Surgical Supplies 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible The cost shares listed above apply when your Provider submits separate bills for the equipment or supplies. Prosthetic limbs (artificial leg or arm) or an Orthotic custom fabricated brace or support designed as a component for a Prosthetic limb are covered the same as any other Medically Necessary items and services and will be subject to the same annual Deductible, Coinsurance, and Copayment as any other service under this Plan. • Wigs Needed After Cancer Treatment Benefit Maximum One wig per Benefit Period. In- and Out-of-Network combined The Plan’s reimbursement for durable medical equipment, orthotics, prosthetics, devices and supplies, and wigs will be based on the Maximum Allowed Amount for a standard item that is Medically Necessary to meet your needs. If you choose to purchase an item with features that exceed what is Medically Necessary, benefits will be limited to the Maximum Allowed Amount for the standard item, and you will be required to pay any costs that exceed the Maximum Allowed Amount. Please check with your Provider or contact us if you have questions about the Maximum Allowed Amount. Emergency Room Services Emergency Room • Emergency Room Facility Charge $250 Copayment per visit then 20% Coinsurance after Deductible Copayment waived if admitted • Emergency Room Doctor Charge (ER physician, radiologist, anesthesiologist, surgeon) 20% Coinsurance after Deductible • Emergency Room Doctor Charge (Mental Health / Substance Use Disorder) 20% Coinsurance after Deductible • Other Facility Charges (including diagnostic x- ray and lab services, medical supplies) 20% Coinsurance after Deductible • Advanced Diagnostic Imaging (including MRIs, CAT scans) 20% Coinsurance after Deductible As described in the “Consolidated Appropriations Act of 2021 Notice” at the front of this Booklet, for Emergency Services, Out-of-Network Providers may only bill you for any applicable Copayments, Deductible and Coinsurance and may not bill you for any charges over the Plan’s Maximum Allowed Amount until the treating Out-of-Network Provider has determined you are stable and followed the notice and consent process. Please refer to the Notice at the beginning of this Booklet for more details. Habilitative Services Benefits are based on the setting in which Covered Services are received.
 Benefit Booklet: Plan 2 Page 19 Page 21
Benefit Booklet: Plan 2 Page 19 Page 21