
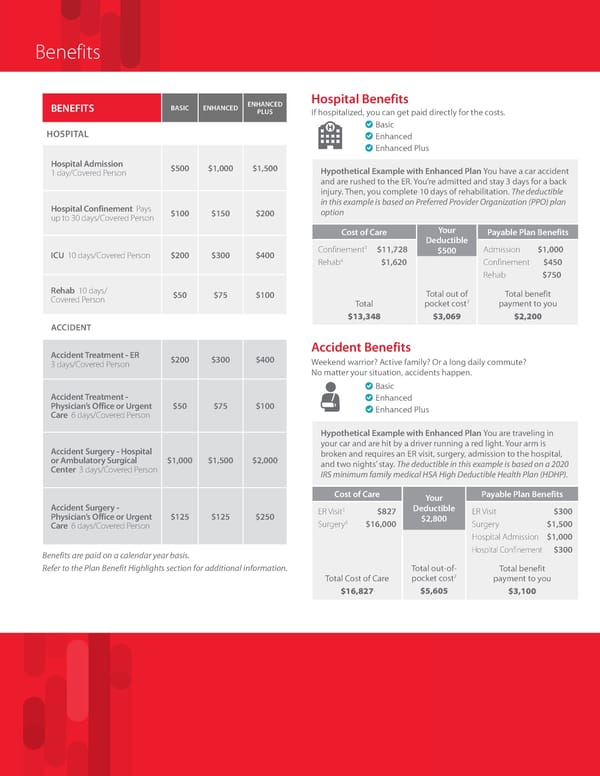
Benefits ENHANCED Hospital Benefits BENEFITS BASIC ENHANCED PLUS If hospitalized, you can get paid directly for the costs. Basic HOSPITAL Enhanced Enhanced Plus Hospital Admission $500 $1,000 $1,500 Hypothetical Example with Enhanced Plan You have a car accident 1 day/Covered Person and are rushed to the ER. You’re admitted and stay 3 days for a back injury. Then, you complete 10 days of rehabilitation. The deductible Hospital Confinement Pays in this example is based on Preferred Provider Organization (PPO) plan up to 30 days/Covered Person $100 $150 $200 option Cost of Care Your Payable Plan Benefits Deductible 3 $11,728 ICU 10 days/Covered Person $200 $300 $400 Confinement $500 Admission $1,000 4 Rehab $1,620 Confinement $450 Rehab $750 Rehab 10 days/ $50 $75 $100 Total out of Total benefit Covered Person pocket cost7 payment to you Total $13,348 $3,069 $2,200 ACCIDENT Accident Treatment - ER Accident Benefits 3 days/Covered Person $200 $300 $400 Weekend warrior? Active family? Or a long daily commute? No matter your situation, accidents happen. Basic Accident Treatment - Enhanced Physician’s Office or Urgent $50 $75 $100 Enhanced Plus Care 6 days/Covered Person Hypothetical Example with Enhanced Plan You are traveling in Accident Surgery - Hospital your car and are hit by a driver running a red light. Your arm is or Ambulatory Surgical $1,000 $1,500 $2,000 broken and requires an ER visit, surgery, admission to the hospital, Center 3 days/Covered Person and two nights’ stay. The deductible in this example is based on a 2020 IRS minimum family medical HSA High Deductible Health Plan (HDHP). Cost of Care Your Payable Plan Benefits Accident Surgery - 5 Deductible Physician’s Office or Urgent $125 $125 $250 ER Visit $827 $2,800 ER Visit $300 6 Care 6 days/Covered Person Surgery $16,000 Surgery $1,500 Hospital Admission $1,000 Benefits are paid on a calendar year basis. Hospital Confinement $300 Refer to the Plan Benefit Highlights section for additional information. Total out-of- Total benefit Total Cost of Care pocket cost7 payment to you $16,827 $5,605 $3,100
 Group Hospital Indemnity IN Page 1 Page 3
Group Hospital Indemnity IN Page 1 Page 3