
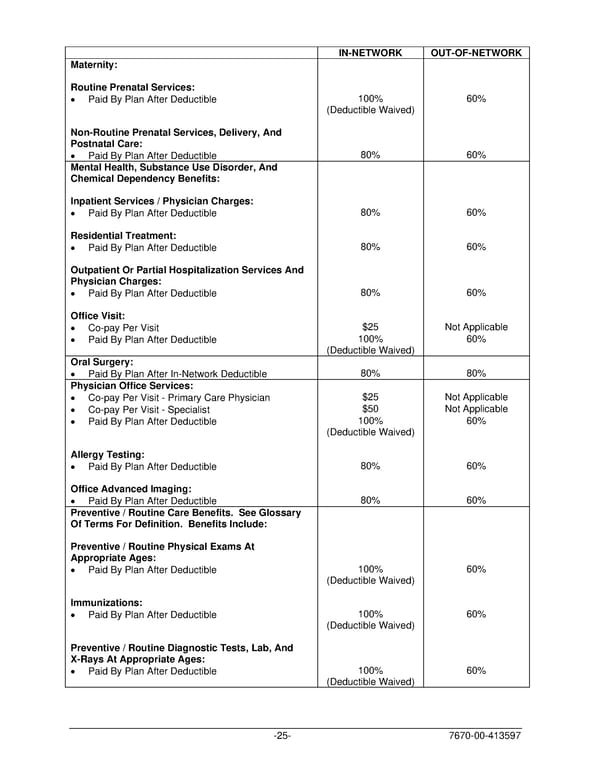
IN-NETWORK OUT-OF-NETWORK Maternity: Routine Prenatal Services: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Non-Routine Prenatal Services, Delivery, And Postnatal Care: • Paid By Plan After Deductible 80% 60% Mental Health, Substance Use Disorder, And Chemical Dependency Benefits: Inpatient Services / Physician Charges: • Paid By Plan After Deductible 80% 60% Residential Treatment: • Paid By Plan After Deductible 80% 60% Outpatient Or Partial Hospitalization Services And Physician Charges: • Paid By Plan After Deductible 80% 60% Office Visit: • Co-pay Per Visit $25 Not Applicable • Paid By Plan After Deductible 100% 60% (Deductible Waived) Oral Surgery: • Paid By Plan After In-Network Deductible 80% 80% Physician Office Services: • Co-pay Per Visit - Primary Care Physician $25 Not Applicable • Co-pay Per Visit - Specialist $50 Not Applicable • Paid By Plan After Deductible 100% 60% (Deductible Waived) Allergy Testing: • Paid By Plan After Deductible 80% 60% Office Advanced Imaging: • Paid By Plan After Deductible 80% 60% Preventive / Routine Care Benefits. See Glossary Of Terms For Definition. Benefits Include: Preventive / Routine Physical Exams At Appropriate Ages: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Immunizations: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Preventive / Routine Diagnostic Tests, Lab, And X-Rays At Appropriate Ages: • Paid By Plan After Deductible 100% 60% (Deductible Waived) -25- 7670-00-413597
 PLAN 01 01 2024 00 Page 27 Page 29
PLAN 01 01 2024 00 Page 27 Page 29