
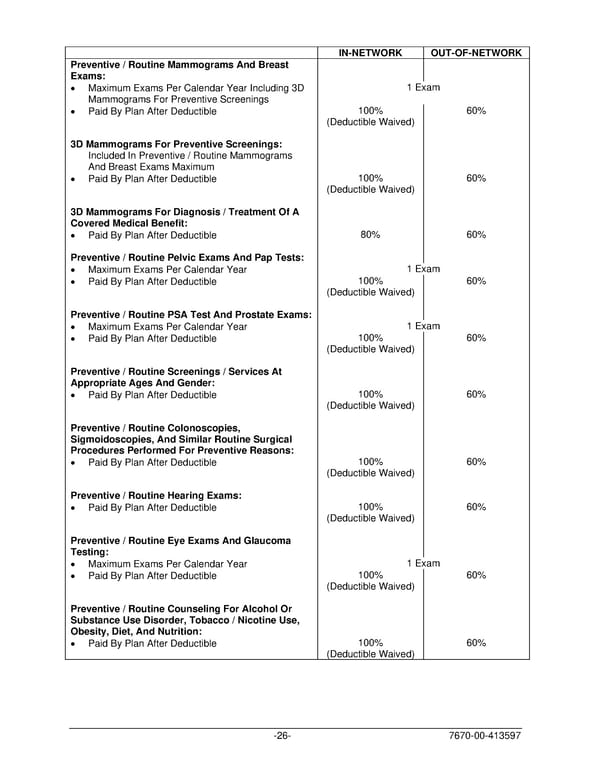
IN-NETWORK OUT-OF-NETWORK Preventive / Routine Mammograms And Breast Exams: • Maximum Exams Per Calendar Year Including 3D 1 Exam Mammograms For Preventive Screenings • Paid By Plan After Deductible 100% 60% (Deductible Waived) 3D Mammograms For Preventive Screenings: Included In Preventive / Routine Mammograms And Breast Exams Maximum • Paid By Plan After Deductible 100% 60% (Deductible Waived) 3D Mammograms For Diagnosis / Treatment Of A Covered Medical Benefit: • Paid By Plan After Deductible 80% 60% Preventive / Routine Pelvic Exams And Pap Tests: • Maximum Exams Per Calendar Year 1 Exam • Paid By Plan After Deductible 100% 60% (Deductible Waived) Preventive / Routine PSA Test And Prostate Exams: • Maximum Exams Per Calendar Year 1 Exam • Paid By Plan After Deductible 100% 60% (Deductible Waived) Preventive / Routine Screenings / Services At Appropriate Ages And Gender: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Preventive / Routine Colonoscopies, Sigmoidoscopies, And Similar Routine Surgical Procedures Performed For Preventive Reasons: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Preventive / Routine Hearing Exams: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Preventive / Routine Eye Exams And Glaucoma Testing: • Maximum Exams Per Calendar Year 1 Exam • Paid By Plan After Deductible 100% 60% (Deductible Waived) Preventive / Routine Counseling For Alcohol Or Substance Use Disorder, Tobacco / Nicotine Use, Obesity, Diet, And Nutrition: • Paid By Plan After Deductible 100% 60% (Deductible Waived) -26- 7670-00-413597
 PLAN 01 01 2024 00 Page 28 Page 30
PLAN 01 01 2024 00 Page 28 Page 30