
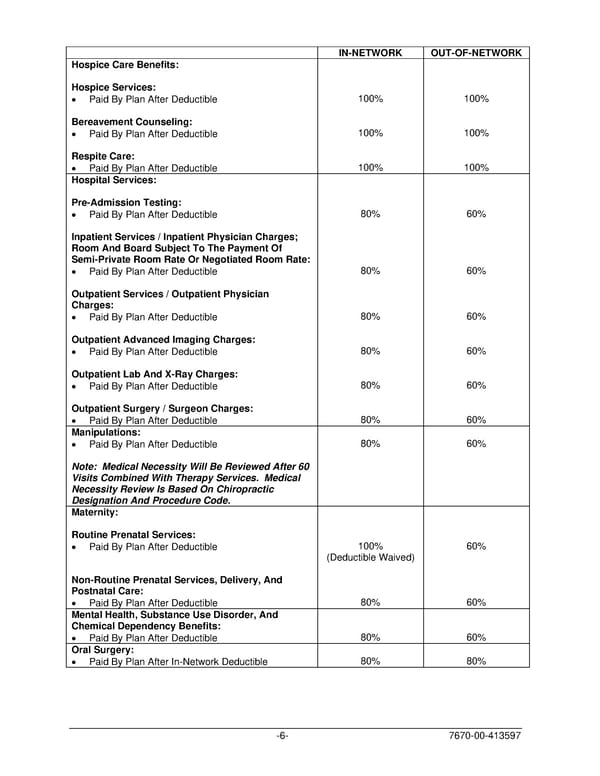
IN-NETWORK OUT-OF-NETWORK Hospice Care Benefits: Hospice Services: • Paid By Plan After Deductible 100% 100% Bereavement Counseling: • Paid By Plan After Deductible 100% 100% Respite Care: • Paid By Plan After Deductible 100% 100% Hospital Services: Pre-Admission Testing: • Paid By Plan After Deductible 80% 60% Inpatient Services / Inpatient Physician Charges; Room And Board Subject To The Payment Of Semi-Private Room Rate Or Negotiated Room Rate: • Paid By Plan After Deductible 80% 60% Outpatient Services / Outpatient Physician Charges: • Paid By Plan After Deductible 80% 60% Outpatient Advanced Imaging Charges: • Paid By Plan After Deductible 80% 60% Outpatient Lab And X-Ray Charges: • Paid By Plan After Deductible 80% 60% Outpatient Surgery / Surgeon Charges: • Paid By Plan After Deductible 80% 60% Manipulations: • Paid By Plan After Deductible 80% 60% Note: Medical Necessity Will Be Reviewed After 60 Visits Combined With Therapy Services. Medical Necessity Review Is Based On Chiropractic Designation And Procedure Code. Maternity: Routine Prenatal Services: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Non-Routine Prenatal Services, Delivery, And Postnatal Care: • Paid By Plan After Deductible 80% 60% Mental Health, Substance Use Disorder, And Chemical Dependency Benefits: • Paid By Plan After Deductible 80% 60% Oral Surgery: • Paid By Plan After In-Network Deductible 80% 80% -6- 7670-00-413597
 PLAN 01 01 2024 00 Page 8 Page 10
PLAN 01 01 2024 00 Page 8 Page 10