
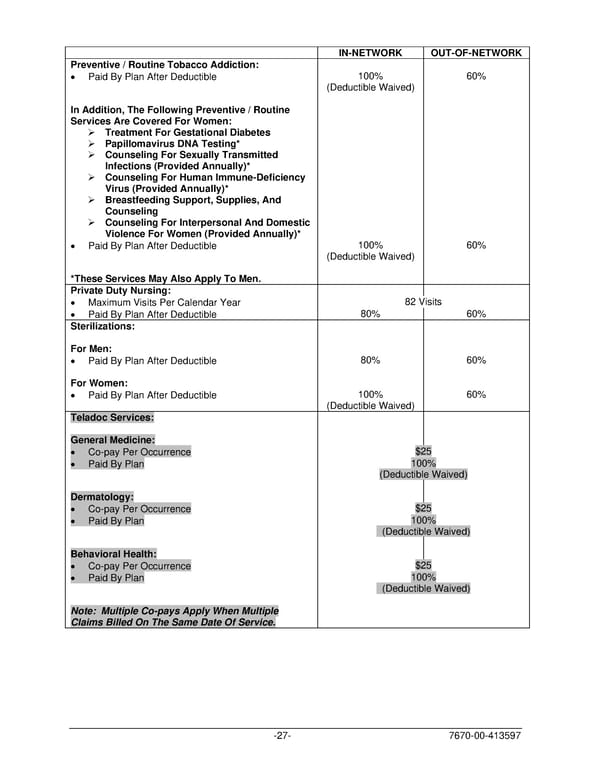
IN-NETWORK OUT-OF-NETWORK Preventive / Routine Tobacco Addiction: • Paid By Plan After Deductible 100% 60% (Deductible Waived) In Addition, The Following Preventive / Routine Services Are Covered For Women: ➢ Treatment For Gestational Diabetes ➢ Papillomavirus DNA Testing* ➢ Counseling For Sexually Transmitted Infections (Provided Annually)* ➢ Counseling For Human Immune-Deficiency Virus (Provided Annually)* ➢ Breastfeeding Support, Supplies, And Counseling ➢ Counseling For Interpersonal And Domestic Violence For Women (Provided Annually)* • Paid By Plan After Deductible 100% 60% (Deductible Waived) *These Services May Also Apply To Men. Private Duty Nursing: • Maximum Visits Per Calendar Year 82 Visits • Paid By Plan After Deductible 80% 60% Sterilizations: For Men: • Paid By Plan After Deductible 80% 60% For Women: • Paid By Plan After Deductible 100% 60% (Deductible Waived) Teladoc Services: General Medicine: • Co-pay Per Occurrence $25 • Paid By Plan 100% (Deductible Waived) Dermatology: • Co-pay Per Occurrence $25 • Paid By Plan 100% (Deductible Waived) Behavioral Health: • Co-pay Per Occurrence $25 • Paid By Plan 100% (Deductible Waived) Note: Multiple Co-pays Apply When Multiple Claims Billed On The Same Date Of Service. -27- 7670-00-413597
 PLAN 01 01 2024 00 Page 29 Page 31
PLAN 01 01 2024 00 Page 29 Page 31