
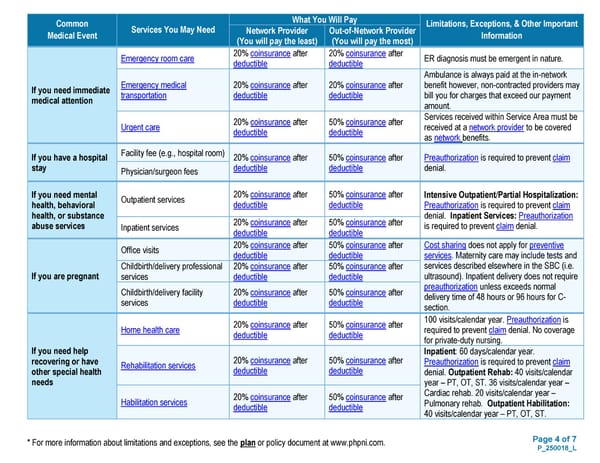
Page 4 of 7 P_250018_L * For more information about limitations and exceptions, see the plan or policy document at www.phpni.com. Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information Network Provider (You will pay the least) Out-of-Network Provider (You will pay the most) If you need immediate medical attention Emergency room care 20% coinsurance after deductible 20% coinsurance after deductible ER diagnosis must be emergent in nature. Emergency medical transportation 20% coinsurance after deductible 20% coinsurance after deductible Ambulance is always paid at the in-network benefit however, non-contracted providers may bill you for charges that exceed our payment amount. Urgent care 20% coinsurance after deductible 50% coinsurance after deductible Services received within Service Area must be received at a network provider to be covered as network benefits. If you have a hospital stay Facility fee (e.g., hospital room) 20% coinsurance after deductible 50% coinsurance after deductible Preauthorization is required to prevent claim denial. Physician/surgeon fees If you need mental health, behavioral health, or substance abuse services Outpatient services 20% coinsurance after deductible 50% coinsurance after deductible Intensive Outpatient/Partial Hospitalization: Preauthorization is required to prevent claim denial. Inpatient Services: Preauthorization is required to prevent claim denial. Inpatient services 20% coinsurance after deductible 50% coinsurance after deductible If you are pregnant Office visits 20% coinsurance after deductible 50% coinsurance after deductible Cost sharing does not apply for preventive services. Maternity care may include tests and services described elsewhere in the SBC (i.e. ultrasound). Inpatient delivery does not require preauthorization unless exceeds normal delivery time of 48 hours or 96 hours for C- section. Childbirth/delivery professional services 20% coinsurance after deductible 50% coinsurance after deductible Childbirth/delivery facility services 20% coinsurance after deductible 50% coinsurance after deductible If you need help recovering or have other special health needs Home health care 20% coinsurance after deductible 50% coinsurance after deductible 100 visits/calendar year. Preauthorization is required to prevent claim denial. No coverage for private-duty nursing. Rehabilitation services 20% coinsurance after deductible 50% coinsurance after deductible Inpatient: 60 days/calendar year. Preauthorization is required to prevent claim denial. Outpatient Rehab: 40 visits/calendar year – PT, OT, ST. 36 visits/calendar year – Cardiac rehab. 20 visits/calendar year – Pulmonary rehab. Outpatient Habilitation: 40 visits/calendar year – PT, OT, ST. Habilitation services 20% coinsurance after deductible 50% coinsurance after deductible
 Plan 1 SBC Page 3 Page 5
Plan 1 SBC Page 3 Page 5