
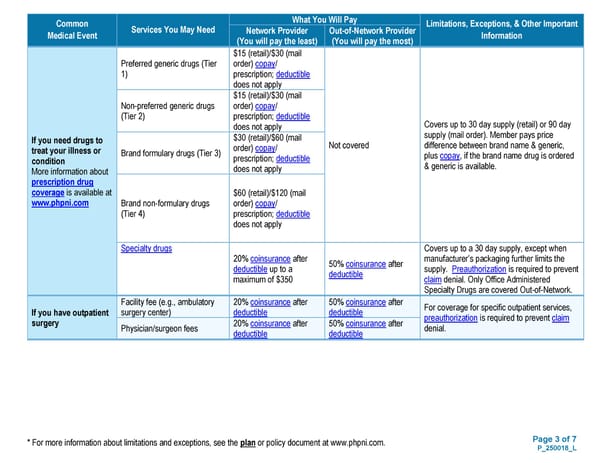
Page 3 of 7 P_250018_L * For more information about limitations and exceptions, see the plan or policy document at www.phpni.com. Common Medical Event Services You May Need What You Will Pay Limitations, Exceptions, & Other Important Information Network Provider (You will pay the least) Out-of-Network Provider (You will pay the most) If you need drugs to treat your illness or condition More information about prescription drug coverage is available at www.phpni.com Preferred generic drugs (Tier 1) $15 (retail)/$30 (mail order) copay/ prescription; deductible does not apply Not covered Covers up to 30 day supply (retail) or 90 day supply (mail order). Member pays price difference between brand name & generic, plus copay, if the brand name drug is ordered & generic is available. Non-preferred generic drugs (Tier 2) $15 (retail)/$30 (mail order) copay/ prescription; deductible does not apply Brand formulary drugs (Tier 3) $30 (retail)/$60 (mail order) copay/ prescription; deductible does not apply Brand non-formulary drugs (Tier 4) $60 (retail)/$120 (mail order) copay/ prescription; deductible does not apply Specialty drugs 20% coinsurance after deductible up to a maximum of $350 50% coinsurance after deductible Covers up to a 30 day supply, except when manufacturer’s packaging further limits the supply. Preauthorization is required to prevent claim denial. Only Office Administered Specialty Drugs are covered Out-of-Network. If you have outpatient surgery Facility fee (e.g., ambulatory surgery center) 20% coinsurance after deductible 50% coinsurance after deductible For coverage for specific outpatient services, preauthorization is required to prevent claim denial. Physician/surgeon fees 20% coinsurance after deductible 50% coinsurance after deductible
 Plan 1 SBC Page 2 Page 4
Plan 1 SBC Page 2 Page 4