
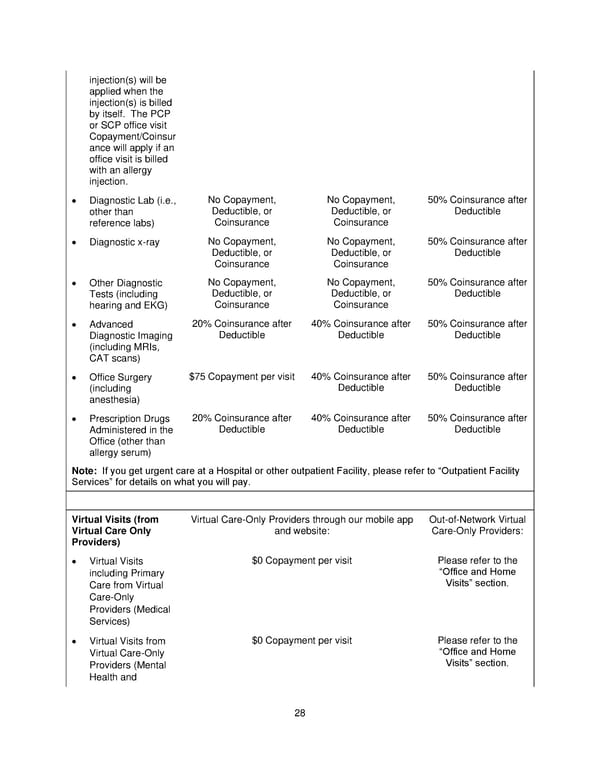
28 injection(s) will be applied when the injection(s) is billed by itself. The PCP or SCP office visit Copayment/Coinsur ance will apply if an office visit is billed with an allergy injection. Diagnostic Lab ( i.e., other than reference labs) No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible Diagnostic x - ray No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible Other Diagnostic Tests (including hearing and EKG) No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible Advanced Diagnostic Imaging (including MRIs, CAT scans) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible Office Surgery (including anesthesia) $75 Copayment per visit 40% Coinsurance after Deductible 50% Coinsurance after Deductible Prescription Drugs Administered in the Office (other than allergy serum) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible Note: If you get urgent care at a Hospital or other outpatient Facility, please refer to Outpatient Facility Services for details on what you will pay. Virtual Visits ( from Virtual Care Only Providers ) Virtual Care - Only Providers through our mobile app and website: Out - of - Network Virtual Care - Only Providers: Virtual Visits including Primary Care from Virtual Care - Only Providers (Medical Services) $0 Copayment per visit Please refer to the Office and Home Visits section. Virtual Visits from Virtual Care - Only Provider s (Mental Health and $0 Copayment per visit Please refer to the Office and Home Visits section.
 Plan 1 SPD 2025 Page 28 Page 30
Plan 1 SPD 2025 Page 28 Page 30