
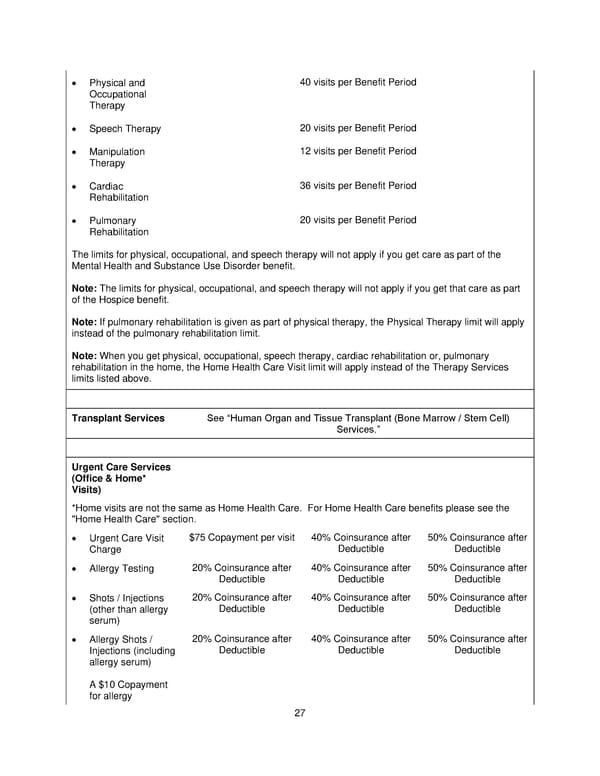
27 Physical and Occupational Therapy 40 visits per Benefit Period Speech Therapy 20 visits per Benefit Period Manipulation Therapy 12 visits per Benefit Period Cardiac Rehabilitation 36 visits per Benefit Period Pulmonary Rehabilitation 20 visits per Benefit Period The limits for physical, occupational, and speech therapy will not apply if you get care as part of the Mental Health and Substance Use Disorder benefit. Note: The limits for physical, occupational, and speech therapy will not apply if you get that care as part of the Hospice benefit. Note: If pulmonary rehabilitation is given as part of physical therapy, the Physical Therapy limit will apply instead of the p ulmonary r ehabilitation limit. Note: When you get physical, occupational, speech therapy , cardiac rehabilitation or , pulmonary rehabilitation in the home, the Home Health Care Visit limit will apply instead of the Therapy Services limits listed above. Transplant Services See Human Organ and Tissue Transplant (Bone Marrow / Stem Cell) Services. Urgent Care Services (Office & Home* Visits) * Home visits are not the same as Home Health Care. For Home Health Care benefits please see the "Home Health Care" section. Urgent Care Visit Charge $75 Copayment per visit 40% Coinsurance after Deductible 50% Coinsurance after Deductible Allergy Testing 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible Shots / Injections (other than allergy serum) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible Allergy Shots / Injections (including allergy serum) A $10 Copayment for allergy 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible
 Plan 1 SPD 2025 Page 27 Page 29
Plan 1 SPD 2025 Page 27 Page 29