
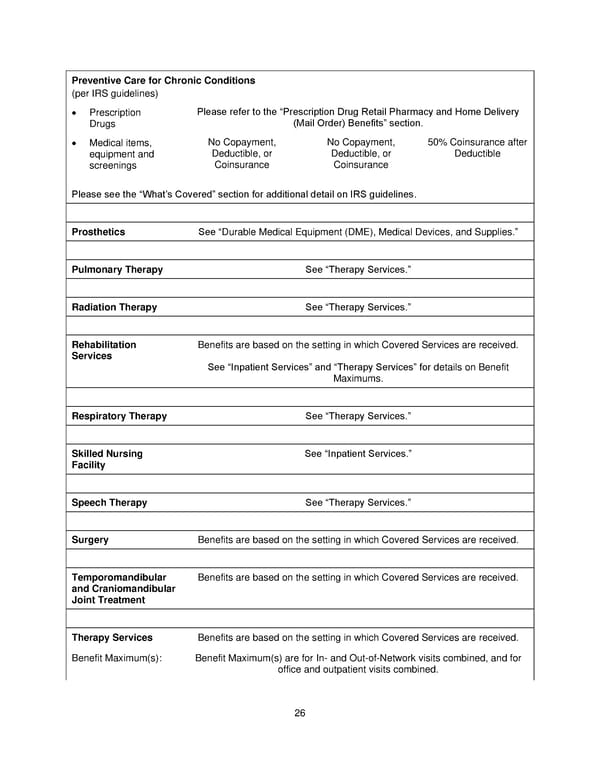
26 Preventive Care for Chronic Conditions (per IRS guidelines) Prescription Drugs Please refer to the Prescription Drug Retail Pharmacy and Home Delivery (Mail Order) Benefits section. Medical items, equipment and screenings No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible Please see the Whats Covered section for additional detail on IRS guidelines . Prosthetics See Durable Medical Equipment (DME ), Medical Devices, and Supplies. Pulmonary Therapy See Therapy Services. Radiation Therapy See Therapy Services. Rehabilitation Services Benefits are based on the setting in which Covered Services are received. See Inpatient Services and Therapy Services for details on Benefit Maximums. Respiratory Therapy See Therapy Services. Skilled Nursing Facility See Inpatient Services. Speech Therapy See Therapy Services. Surgery Benefits are based on the setting in which Covered Services are received. Temporomandibular and Craniomandibular Joint Treatment Benefits are based on the setting in which Covered Services are received. Therapy Services Benefits are based on the setting in which Covered Services are received. Benefit Maximum(s) : Benefit Maximum(s) are for In - and Out - of - Network visits combined, and for office and outpatient visits combined.
 Plan 1 SPD 2025 Page 26 Page 28
Plan 1 SPD 2025 Page 26 Page 28