
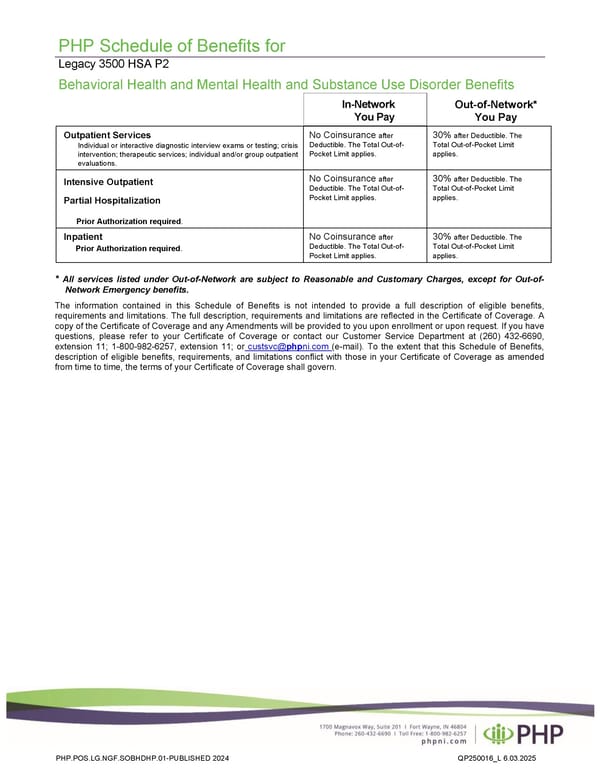
PHP Schedule of Benefits for Legacy 3500 HSA P2 Behavioral Health and Mental Health and Substance Use Disorder Benefits In-Network You Pay Outpatient Services Individual or interactive diagnostic interview exams or testing; crisis intervention; therapeutic services; individual and/or group outpatient evaluations. No Coinsurance after Deductible. The Total Out-of- Pocket Limit applies. 30% after Deductible. The Total Out-of-Pocket Limit applies. Intensive Outpatient Partial Hospitalization Prior Authorization required. No Coinsurance after Deductible. The Total Out-of- Pocket Limit applies. 30% after Deductible. The Total Out-of-Pocket Limit applies. Inpatient Prior Authorization required. No Coinsurance after Deductible. The Total Out-of- Pocket Limit applies. 30% after Deductible. The Total Out-of-Pocket Limit applies. * All services listed under Out-of-Network are subject to Reasonable and Customary Charges, except for Out-of- Network Emergency benefits. The information contained in this Schedule of Benefits is not intended to provide a full description of eligible benefits, requirements and limitations. The full description, requirements and limitations are reflected in the Certificate of Coverage. A copy of the Certificate of Coverage and any Amendments will be provided to you upon enrollment or upon request. If you have questions, please refer to your Certificate of Coverage or contact our Customer Service Department at (260) 432-6690, extension 11; 1-800-982-6257, extension 11; or custsvc@phpni.com (e-mail). To the extent that this Schedule of Benefits, description of eligible benefits, requirements, and limitations conflict with those in your Certificate of Coverage as amended from time to time, the terms of your Certificate of Coverage shall govern. PHP.POS.LG.NGF.SOBHDHP.01-PUBLISHED 2024 QP250016_L 6.03.2025 Out-of-Network* You Pay
 Plan 2 - 3500 Page 5
Plan 2 - 3500 Page 5