
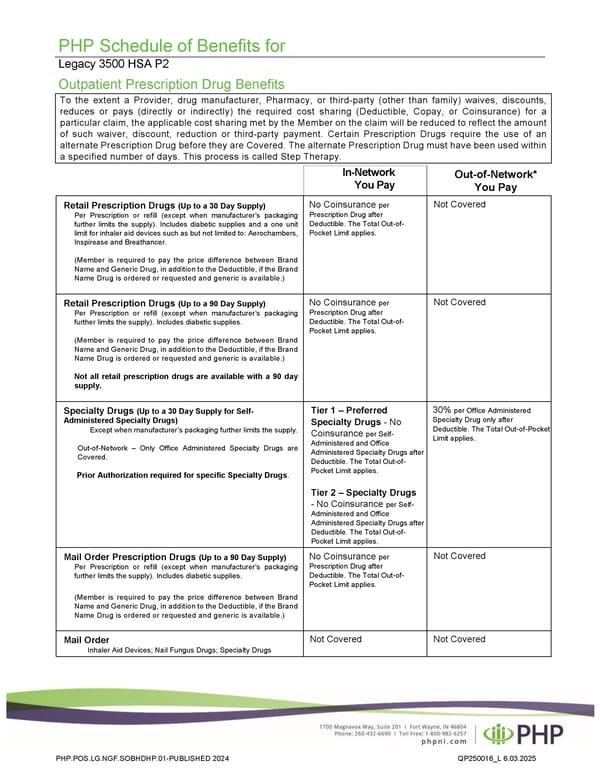
PHP Schedule of Benefits for Legacy 3500 HSA P2 Outpatient Prescription Drug Benefits To the extent a Provider, drug manufacturer, Pharmacy, or third-party (other than family) waives, discounts, reduces or pays (directly or indirectly) the required cost sharing (Deductible, Copay, or Coinsurance) for a particular claim, the applicable cost sharing met by the Member on the claim will be reduced to reflect the amount of such waiver, discount, reduction or third-party payment. Certain Prescription Drugs require the use of an alternate Prescription Drug before they are Covered. The alternate Prescription Drug must have been used within a specified number of days. This process is called Step Therapy. In-Network You Pay Retail Prescription Drugs (Up to a 30 Day Supply) Per Prescription or refill (except when manufacturer’s packaging further limits the supply). Includes diabetic supplies and a one unit limit for inhaler aid devices such as but not limited to: Aerochambers, Inspirease and Breathancer. (Member is required to pay the price difference between Brand Name and Generic Drug, in addition to the Deductible, if the Brand Name Drug is ordered or requested and generic is available.) No Coinsurance per Prescription Drug after Deductible. The Total Out-of- Pocket Limit applies. Not Covered Retail Prescription Drugs (Up to a 90 Day Supply) Per Prescription or refill (except when manufacturer’s packaging further limits the supply). Includes diabetic supplies. (Member is required to pay the price difference between Brand Name and Generic Drug, in addition to the Deductible, if the Brand Name Drug is ordered or requested and generic is available.) Not all retail prescription drugs are available with a 90 day supply. No Coinsurance per Prescription Drug after Deductible. The Total Out-of- Pocket Limit applies. Not Covered Specialty Drugs (Up to a 30 Day Supply for Self- Administered Specialty Drugs) Except when manufacturer’s packaging further limits the supply. Out-of-Network – Only Office Administered Specialty Drugs are Covered. Prior Authorization required for specific Specialty Drugs. Tier 1 – Preferred Specialty Drugs - No Coinsurance per Self- Administered and Office Administered Specialty Drugs after Deductible. The Total Out-of- Pocket Limit applies. Tier 2 – Specialty Drugs - No Coinsurance per Self- Administered and Office Administered Specialty Drugs after Deductible. The Total Out-of- Pocket Limit applies. 30% per Office Administered Specialty Drug only after Deductible. The Total Out-of-Pocket Limit applies. Mail Order Prescription Drugs (Up to a 90 Day Supply) Per Prescription or refill (except when manufacturer’s packaging further limits the supply). Includes diabetic supplies. (Member is required to pay the price difference between Brand Name and Generic Drug, in addition to the Deductible, if the Brand Name Drug is ordered or requested and generic is available.) No Coinsurance per Prescription Drug after Deductible. The Total Out-of- Pocket Limit applies. Not Covered Mail Order Inhaler Aid Devices; Nail Fungus Drugs; Specialty Drugs Not Covered Not Covered PHP.POS.LG.NGF.SOBHDHP.01-PUBLISHED 2024 QP250016_L 6.03.2025 Out-of-Network* You Pay
 Plan 2 - 3500 Page 4 Page 6
Plan 2 - 3500 Page 4 Page 6