
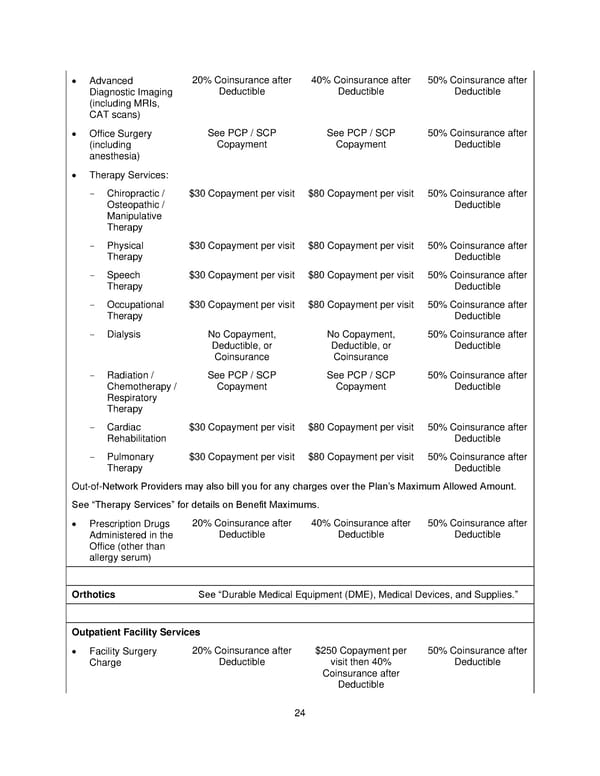
• Advanced 20% Coinsurance after 40% Coinsurance after 50% Coinsurance after Diagnostic Imaging Deductible Deductible Deductible (including MRIs, CAT scans) • Office Surgery See PCP / SCP See PCP / SCP 50% Coinsurance after (including Copayment Copayment Deductible anesthesia) • Therapy Services: - Chiropractic / $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Osteopathic / Deductible Manipulative Therapy - Physical $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Therapy Deductible - Speech $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Therapy Deductible - Occupational $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Therapy Deductible - Dialysis No Copayment, No Copayment, 50% Coinsurance after Deductible, or Deductible, or Deductible Coinsurance Coinsurance - Radiation / See PCP / SCP See PCP / SCP 50% Coinsurance after Chemotherapy / Copayment Copayment Deductible Respiratory Therapy - Cardiac $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Rehabilitation Deductible - Pulmonary $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Therapy Deductible Out-of-Network Providers may also bill you for any charges over the Plan’s Maximum Allowed Amount. See “Therapy Services” for details on Benefit Maximums. • Prescription Drugs 20% Coinsurance after 40% Coinsurance after 50% Coinsurance after Administered in the Deductible Deductible Deductible Office (other than allergy serum) Orthotics See “Durable Medical Equipment (DME), Medical Devices, and Supplies.” Outpatient Facility Services • Facility Surgery 20% Coinsurance after $250 Copayment per 50% Coinsurance after Charge Deductible visit then 40% Deductible Coinsurance after Deductible 24
 Plan 2 SPD 2025 Page 24 Page 26
Plan 2 SPD 2025 Page 24 Page 26