
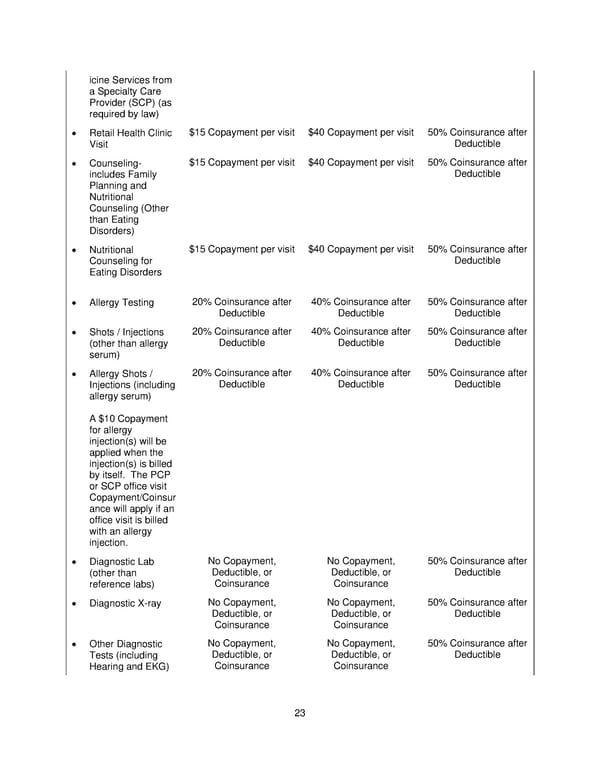
icine Services from a Specialty Care Provider (SCP) (as required by law) • Retail Health Clinic $15 Copayment per visit $40 Copayment per visit 50% Coinsurance after Visit Deductible • Counseling- $15 Copayment per visit $40 Copayment per visit 50% Coinsurance after includes Family Deductible Planning and Nutritional Counseling (Other than Eating Disorders) • Nutritional $15 Copayment per visit $40 Copayment per visit 50% Coinsurance after Counseling for Deductible Eating Disorders • Allergy Testing 20% Coinsurance after 40% Coinsurance after 50% Coinsurance after Deductible Deductible Deductible • Shots / Injections 20% Coinsurance after 40% Coinsurance after 50% Coinsurance after (other than allergy Deductible Deductible Deductible serum) • Allergy Shots / 20% Coinsurance after 40% Coinsurance after 50% Coinsurance after Injections (including Deductible Deductible Deductible allergy serum) A $10 Copayment for allergy injection(s) will be applied when the injection(s) is billed by itself. The PCP or SCP office visit Copayment/Coinsur ance will apply if an office visit is billed with an allergy injection. • Diagnostic Lab No Copayment, No Copayment, 50% Coinsurance after (other than Deductible, or Deductible, or Deductible reference labs) Coinsurance Coinsurance • Diagnostic X-ray No Copayment, No Copayment, 50% Coinsurance after Deductible, or Deductible, or Deductible Coinsurance Coinsurance • Other Diagnostic No Copayment, No Copayment, 50% Coinsurance after Tests (including Deductible, or Deductible, or Deductible Hearing and EKG) Coinsurance Coinsurance 23
 Plan 2 SPD 2025 Page 23 Page 25
Plan 2 SPD 2025 Page 23 Page 25