
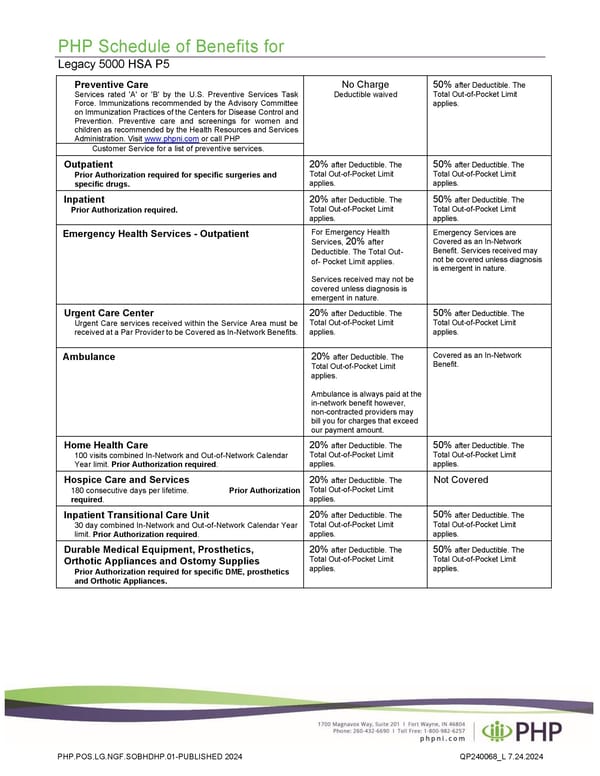
PHP Schedule of Benefits for Legacy 5000 HSA P5 Preventive Care Services rated 'A' or 'B' by the U.S. Preventive Services Task Force. Immunizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screenings for women and children as recommended by the Health Resources and Services Administration. Visit www.phpni.com or call PHP No Charge Deductible waived 50% after Deductible. The Total Out-of-Pocket Limit applies. Customer Service for a list of preventive services. Outpatient Prior Authorization required for specific surgeries and specific drugs. 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. Inpatient Prior Authorization required. 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. Emergency Health Services - Outpatient For Emergency Health Services, 20% after Deductible. The Total Out- of- Pocket Limit applies. Services received may not be covered unless diagnosis is emergent in nature. Emergency Services are Covered as an In-Network Benefit. Services received may not be covered unless diagnosis is emergent in nature. Urgent Care Center Urgent Care services received within the Service Area must be received at a Par Provider to be Covered as In-Network Benefits. 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. Ambulance 20% after Deductible. The Total Out-of-Pocket Limit applies. Ambulance is always paid at the in-network benefit however, non-contracted providers may bill you for charges that exceed our payment amount. Covered as an In-Network Benefit. Home Health Care 100 visits combined In-Network and Out-of-Network Calendar Year limit. Prior Authorization required. 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. Hospice Care and Services 180 consecutive days per lifetime. Prior Authorization required. 20% after Deductible. The Total Out-of-Pocket Limit applies. Not Covered Inpatient Transitional Care Unit 30 day combined In-Network and Out-of-Network Calendar Year limit. Prior Authorization required. 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. Durable Medical Equipment, Prosthetics, Orthotic Appliances and Ostomy Supplies Prior Authorization required for specific DME, prosthetics and Orthotic Appliances. 20% after Deductible. The Total Out-of-Pocket Limit applies. 50% after Deductible. The Total Out-of-Pocket Limit applies. PHP.POS.LG.NGF.SOBHDHP.01-PUBLISHED 2024 QP240068_L 7.24.2024
 Plan 3 - 6000 Page 2 Page 4
Plan 3 - 6000 Page 2 Page 4