
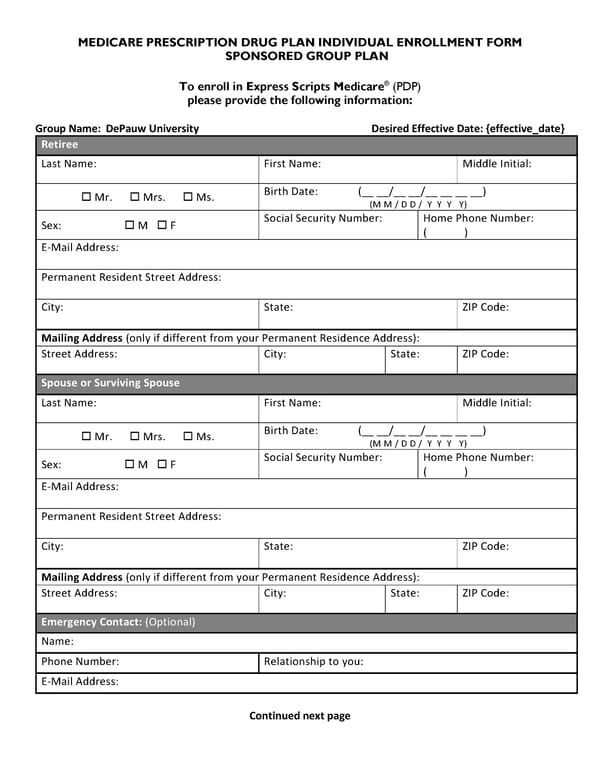
MEDICARE PRESCRIPTION DRUG PLAN INDIVIDUAL ENROLLMENT FORM SPONSORED GROUP PLAN To enroll in Express Scripts Medicare® (PDP) please provide the following information: Group Name: DePauw University Desired Effective Date: {effective_date} Retiree Last Name: First Name: Middle Initial: Mr. Mrs. Ms. Birth Date: (__ __/__ __/__ __ __ __) (M M / D D / Y Y Y Y) Sex: M F Social Security Number: Home Phone Number: ( ) E-Mail Address: Permanent Resident Street Address: City: State: ZIP Code: Mailing Address (only if different from your Permanent Residence Address): Street Address: City: State: ZIP Code: Spouse or Surviving Spouse Last Name: First Name: Middle Initial: Mr. Mrs. Ms. Birth Date: (__ __/__ __/__ __ __ __) (M M / D D / Y Y Y Y) Sex: M F Social Security Number: Home Phone Number: ( ) E-Mail Address: Permanent Resident Street Address: City: State: ZIP Code: Mailing Address (only if different from your Permanent Residence Address): Street Address: City: State: ZIP Code: Emergency Contact: (Optional) Name: Phone Number: Relationship to you: E-Mail Address: Continued next page
 Retiree Medical Plan Election Form Page 2 Page 4
Retiree Medical Plan Election Form Page 2 Page 4