
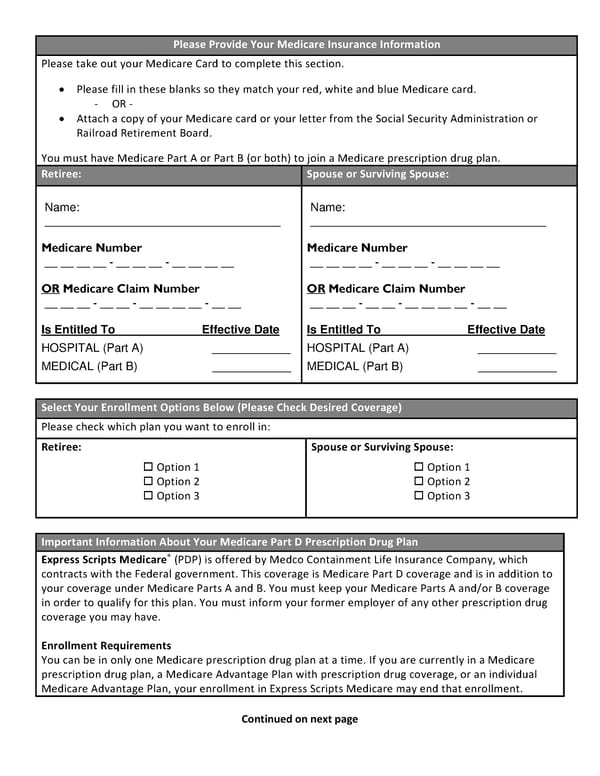
Please Provide Your Medicare Insurance Information Please take out your Medicare Card to complete this section. Please fill in these blanks so they match your red, white and blue Medicare card. - OR - Attach a copy of your Medicare card or your letter from the Social Security Administration or Railroad Retirement Board. You must have Medicare Part A or Part B (or both) to join a Medicare prescription drug plan. Retiree: Spouse or Surviving Spouse: Name: ____________________________________ Medicare Number __ __ __ __ - __ __ __ - __ __ __ __ OR Medicare Claim Number __ __ __ - __ __ - __ __ __ __ - __ __ Is Entitled To Effective Date HOSPITAL (Part A) ____________ MEDICAL (Part B) ____________ Name: ____________________________________ Medicare Number __ __ __ __ - __ __ __ - __ __ __ __ OR Medicare Claim Number __ __ __ - __ __ - __ __ __ __ - __ __ Is Entitled To Effective Date HOSPITAL (Part A) ____________ MEDICAL (Part B) ____________ Select Your Enrollment Options Below (Please Check Desired Coverage) Please check which plan you want to enroll in: Retiree: Option 1 Option 2 Option 3 Spouse or Surviving Spouse: Option 1 Option 2 Option 3 Important Information About Your Medicare Part D Prescription Drug Plan Express Scripts Medicare® (PDP) is offered by Medco Containment Life Insurance Company, which contracts with the Federal government. This coverage is Medicare Part D coverage and is in addition to your coverage under Medicare Parts A and B. You must keep your Medicare Parts A and/or B coverage in order to qualify for this plan. You must inform your former employer of any other prescription drug coverage you may have. Enrollment Requirements You can be in only one Medicare prescription drug plan at a time. If you are currently in a Medicare prescription drug plan, a Medicare Advantage Plan with prescription drug coverage, or an individual Medicare Advantage Plan, your enrollment in Express Scripts Medicare may end that enrollment. Continued on next page
 Retiree Medical Plan Election Form Page 3 Page 5
Retiree Medical Plan Election Form Page 3 Page 5